CYST GAP BRANCHIAL
I Made Nudi Arthana
Cyst gap branchial is Malformation congenital (MK) or disabled born change structure and function of the newborn's organ systems that occur in intrauterine life and are identified before, at or after birth. Birth defects can also be classified as major or minor anomalies depending on the magnitude of the structural and functional abnormalities and the need for medical support or care. Congenital malformations have become a major public health problem because of their significant contribution to newborn mortality and morbidity. birth and infants. The prevalence of MK varies from one area to the area others, but the global prevalence of MK is around 2%- 3%. 1– 3
LITERATURE REVIEW
Definition
Cyst gap branchial is anomaly congenital Which arise from gap first pharynx until fourth. Type cyst gap branchial Which most general appear from the gap second, with anomaly Which originate from gap First, third, And The fourth is less common. Most lesions appear in childhood as a visible punctum on the skin although they may appear as a cyst or neck mass, sometimes misinterpreted as abscess neck. Anomaly gap branchial present in one of three forms: cyst, sinus, or fistula. Cysts have an epithelial lining without an external opening, and thus, may be asymptomatic and only seen incidentally. Such cysts may not appear until adulthood. The sinus tract may communicate either externally with the skin as a visible punctum or internally with the pharynx or larynx, where the punctate opening will be visible only on endoscopy. Branchial cleft fistulas are true communications connecting the pharynx or larynx with the external skin. 11,12
Embryology
The branchial arches develop between the fourth and seventh weeks of gestation. And to form precursor embryology ear And muscle, vessels blood, bone, cartilage, and the mucous membranes of the face, neck, and pharynx. In total, six pairs of branchial arches form on either side of the pharyngeal foregut in craniocaudal succession. Pharyngeal arches The fifth arch is usually only rudimentary, or never forms, so that eventually only five arches form the adult structure. The fifth arch does not contribute to the anatomical structure of the human. Schematically, the sixth arch is often represented as part of the fourth arch because of its small size. 6
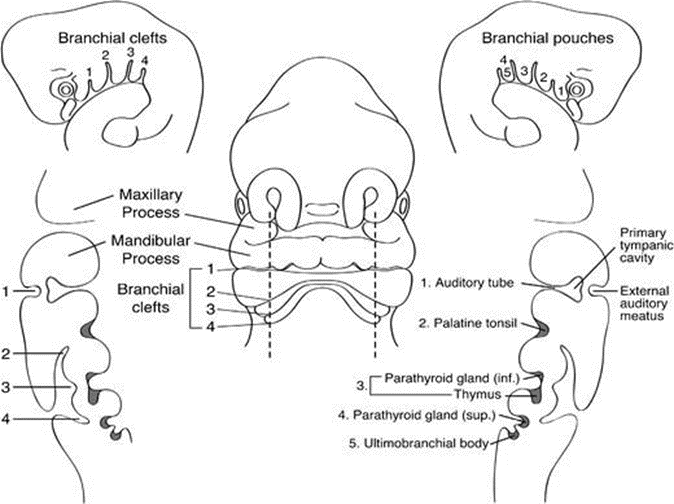
Figure 2.1 Frontal schematic representation of a 5 mm human embryo in the fifth week of gestation. Sagittal section taken through the branchial apparatus shows connection anatomy gap external And pocket internal as well as derivatives of important head and neck structures. The sixth arch is very small and does not visualized as structure Which separated And separated from pocket 4/5.
Each branchial arch is lined externally by an ectodermally lined recess, called the pharyngeal cleft, and internally by an endodermally lined recess, called the pharyngeal pouch. Between the branchial cleft and the pouch is a core of mesenchyme derived from a combination of lateral plate mesoderm, somites, and neural crest cells. The clefts and pouches are gradually obliterated by mesenchymal invasion to form the various adult structures. Each arch has its own central cartilaginous/skeletal supporting elements, an aortic arch artery, and cranial nerves associated with the arch. Curved First supplied by nerve trigeminal (V), arch second by nerve facialist (VII), arch third supplied by nerve glossopharyngeal (IX) and arch fourth And sixth by larynx superior And branch larynx recurrent. vagus nerve (X). Each nerve innervates structures originating from its associated arch.
Each pharyngeal pouch develops into an adult structure. Derivatives of these structures arch pharynx both include fossa tonsils, tonsil palatine, stapes, horn hyoid Which more low, muscles expression face Which close together And base mouth. pouch pharynx third bring up horn Which more big from hyoid, thymus, and the piriform fossa. The precursor of the thymus gland migrates inferiorly and ventrally to the thyroid to fuse in the midline, forming a bilobed structure. The inferior parathyroid glands also develop from the third pharyngeal pouch; the superior parathyroid glands, paradoxically, arise more inferiorly from the fourth pharyngeal pouch. The fourth pharyngeal pouch also contributes to the crest of the piriform fossa, as well as the laryngeal cartilages and muscles. The ultimobranchial body (ultimobranchial body/ultimobranchial gland) is derived from the ventral recess of the fourth pharyngeal pouch, technically the fifth, but one that is rudimentary and fused with Which fourth. This cause cell producer calcitonin ( parafollicular cells / cell C) thyroid gland. The sixth pharyngeal arch contributes to the sternocleidomastoid and trapezius muscles. 6
Etiology and Epidemiology
The etiology of branchial cleft cysts remains controversial. There are four main theories of the origin of branchial cysts postulated to date. These include incomplete obliteration of the branchial mucosa, persistence of pre-cervical sinus remnants, thymo-pharyngeal duct origin and cystic lymph node origin. 7
Cyst gap brachialis is reason general swelling network soft lumps in the neck of young adults. They are usually unilateral and are usually seen on the lateral aspect of the neck. They become clinically apparent in late childhood or early adulthood. In older adults with this presentation, it is important to exclude metastatic lymphadenopathy, lymphoma, or tuberculosis. 7
The true incidence of branchial cleft anomalies in the United States is unknown, although they are relatively frequent. This is likely due to the diversity of anomalies and their presentations that complicate accurate reporting. There is no ethnic or gender predilection. Most branchial cleft anomalies arise from pocket second, whereas pocket First, third, And fourth seldom happened, and 10% from anomaly gap branchial nature bilateral. This usually present in the first decade of life, but if there is no external communication, presentation may be delayed until adulthood. 13
Pathophysiology
Branchial cleft anomalies are formed due to involution of the branchial cleft structure. No complete. Around Sunday fourth pregnancy, cell Christ neural migrate to the future head and neck region, where 6 pairs of branchial arches (pharynx) start develop. Mesoderm covered in a way external by ectoderm and in a way internal coated by endoderm. Usually There is 5 arch branchial, with arch separated by emphasis Which known as gap on ectodermal surface and corresponding pockets on the endodermal surface, producing four pharyngeal slits. The second arch develops caudally and then covers arch third And fourth. Gap Which buried This become an ectoderm-lined cavity that usually undergoes complete involution at gestational age 7 Sunday. If gap No involution or involution No complete, These pathological remnants will form cysts, sinuses, or fistulas at predictable locations according to the origin of the gap. 14,15
Anomaly gap first branchial
Anomaly gap branchial First can happen in where just in throughout the first branchial arch path. It extends from the skin opening in the submandibular triangle, supero-lateral to bone hyoid, go on to area gland saliva parotid to end at the cartilage/bone junction of the external auditory canal. The tract may pass above or below the facial nerve.
Work in 1972 divided the first branchial cleft anomalies into two groups, Type I and Type II, based on presumed pathogenesis with limited application from an imaging perspective;
Type I anomalies are purely ectodermal in origin and present as masses. cystic Which close together with channel hearing external. They is duplication from channel hearing external membrane And contain epithelium squamous but No There is skin or cartilage adnexa.
Type II anomalies may appear as cysts, sinuses, or fistulas in the area corner mandible. They originate from ectodermal and mesodermal, therefore containing squamous epithelium, skin adnexa (hair follicles, sweat and sebaceous glands) and cartilage.
The first branchial cleft anomaly is often misdiagnosed and often untreated. in a way adequate before excised with surgery. They more They are common in women and usually present as a cyst/sinus/fistula between the external auditory canal and the submandibular area. They may present with symptoms cervix And drainage from emphasis like hole in corner mandible. If infected, the drainage may be purulent and there may be associated adenitis in the submandibular region. The first branchial cleft anomaly may also present with an inflammatory mass in the parotid region or present with auricular symptoms and drainage of mucus or pus from the external auditory canal. 6,16
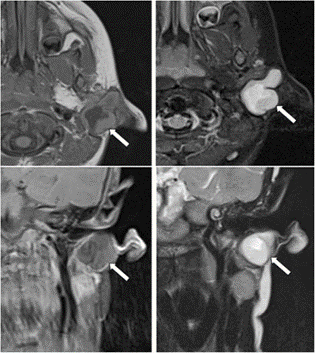
Figure 2.2 MR imaging of a child with purulent ear discharge. Post-contrast T1 axial And coronal (picture hand left) with Axial and coronal STIR images (right hand image) show a thick-walled sinus tract (white arrow) extending into the clinically apparent opening in the left external auditory canal. The tract was surgically excised and was confirmed to represent a first branchial cleft anomaly
On CT imaging, the first branchial cleft anomaly usually appears as a superficial/deep/cystic mass in the parotid salivary gland. As with the anomaly gap branchial other, thickness And improvement wall cyst varies with level inflammation. Anomaly gap branchial First, like anomaly Other branchial clefts, usually do not regress spontaneously and have a tendency to recurrent infection; therefore, surgical excision is recommended for definitive treatment. This involves complete resection while preserving normal structures and using a superficial parotidectomy approach with potential risk of injury to the facial nerve. The degree of the anomaly is usually underestimated and significant skin tracts may be present requiring skin excision and cartilage involved in the external auditory canal. 6
Anomaly gap second branchial
The second most common branchial cleft anomaly presents as a cyst followed by sine And fistula. Part big there is in in room submandibular but can happen in where just in throughout track arcus branchial second Which extending from the skin above the supraclavicular fossa, between the internal and external carotid arteries, to enter the pharynx at the level of the tonsillar fossa. They were previously classified into four distinct subtypes by Bailey in 1929:
Type I – Most superficial and lies along the anterior surface of the sternocleidomastoid deep to the platysma, but does not contact the carotid sheath.
Type II – The most common type in which the branchial cleft cyst is located anterior to the sternocleidomastoid muscle, posterior to the submandibular gland, adjacent and lateral to the carotid sheath.
Type III – Extends medially between the bifurcations of the internal and external carotid arteries, lateral to the pharyngeal wall.
Type IV- Located deep within the carotid sheath within the pharyngeal mucosal space and opens into the pharynx.
Fistulas or cysts in the anterior or lower lateral area of the neck are most likely represent anomaly gap branchial second. Fistula usually diagnosed on infancy/childhood with drainage of secretions or purulent material from an opening at the anterior border of the sternocleidomastoid in the lower third of the neck. Cysts are most commonly diagnosed as painless, compressible lateral neck masses in children/young adults that may become tender and/or enlarge if infected. Histologically, they are filled with yellow fluid cloudy Which contain crystal cholesterol And coated by epithelium stratified squamous. On patient mature, consideration diagnostic main is whether Cystic lesions are metastatic lymph nodes and further imaging is directed to identify the primary neoplastic lesion. This is generally the case if there is no history of chronic neck lumps and no history of recurrent masses after upper respiratory tract infections. Ancillary examinations that can be performed that is with combination imaging cross-sectional [ Magnetic Resonance Imaging (MRI) is the modality of choice] and Positron Emission Tomography- Computed Tomography (PET-CT) before pan-endoscopy and tissue biopsy. Occult papillary thyroid cancer is also known to cause metastasis cystic and can appear on children. Aspiration fluid Which relate with Thyroglobulin levels can help differentiate between them. 6
Anomaly gap branchial third And fourth
The third and fourth branchial cleft anomalies may externally similar to the second branchial cleft anomaly with a skin opening in the supraclavicular region; however, internally, they enter the pharynx through the pyriform sinus beneath the hyoid bone. The third and fourth branchial cleft anomalies are distinguished anatomically by their relationship to the superior laryngeal nerve with the third pharyngeal cleft anomaly above and the fourth pharyngeal cleft anomaly below. The internal opening helps to define their origin and the third branchial cleft sinus arises from the rostral end of the pyriform fossa. Branchial cleft fistula third / channel sine usually appear more beginning from cyst third branchial cleft. Most third branchial cleft cysts present in the posterior cervical space, posterior to the sternocleidomastoid muscle as a painless, fluctuating mass that can grow bigger And become soft If infected. Cyst gap branchial third infected abscess should be considered if the patient presents with an abscess in the posterior triangle of the neck.
The fourth branchial cleft fistula/sinus tract arises from the apex of the pyriform sinus and descends into the lower mediastinum in the path of the tracheoesophageal groove. They are most common in side left For reason Which not yet known and most often present as a sinus tract flows from the apex of the piriform fossa to the aspect on from the left thyroid lobe. As a result, patients may experience recurrent abscesses in the lower anterior neck and/or recurrent suppurative thyroiditis. It is difficult to determine the duct Which appropriate on imaging And This can achieved with test swallow barium which can also be combined with a CT study of the neck after a barium swallow. Because track anatomy, resection complete with operation neck open difficult performed and new endoscopic techniques involving treatment with cauterization have been successfully developed. 6
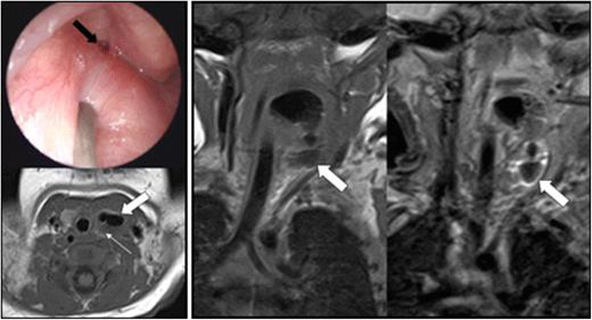
Figure 2.4 This 18-day-old infant presented with intermittent stridor. On examination, left-sided oropharyngeal swelling was identified. Microlaryngobronchoscopy identify opening internal Which arise from the apex of the pyriform sinus (black arrow). Axial and coronal T1 with coronal STIR imaging identified a possible air-containing structure (thick white arrow) extending from the pyriform sinus to the level of the abnormally small left thyroid gland (thin white arrow). This was confirmed surgically by the presence of the fourth branchial cleft sinus tract.
Diagnosis
The history obtained from the patient usually reveals a single mass in the neck, with or without increasing size. The patient may describe symptoms of compression such as dyspnea or dysphagia, or even snoring, if the mass extends to adjacent structures. It may become inflamed and tender after an upper respiratory tract infection. Physical examination usually reveals a smooth, nontender, and nonfluctuant mass . 9
Inspection physique will different depends location cyst branchial cleft . 16
The first branchial cleft cyst is usually a smooth, nontender, fluctuant mass found between the external auditory canal and the submandibular area. Often, it has a skin punctum from which fluid can be drained. The type of contents varies with the parotid gland and facial nerve, and there may be a connection to the middle ear. or outside, so that inspection otological very important in this patient.
The second branchial cleft cyst is usually identified by a hole or punctum of skin at the lower anterior border of the sternocleidomastoid and may be connected to the tonsillar fossa of the pharynx. This type may be close to the glossopharyngeal and hypoglossal nerves and the carotid vessels. The cyst is soft if secondarily infected, And on case Which critical, can cause respiratory tract disorders. If associated with sinus tracts, mucoid or purulent secretions may be present on the skin or in the pharynx.
The third and fourth branchial cleft cysts are rare. They are usually on the left side of the neck or suprasternal notch/clavicular area. They usually appear as a hard mass. or infected cysts that drain into the pyriform sinus or the skin of the outer neck. These fistulas are more likely to occur when infected and may have undergone repeated incision and drainage procedures due to misdiagnosis and subsequent recurrence.
Diagnosis appeal lesi Possible including gland sap clear malignant or benign, malignant or benign neoplasms, cervical adenitis, inflammatory lymphadenopathy, and bacterial and viral infections. The diagnosis can be confirmed by fine-needle aspirate cytology, which usually reveals stratified squamous epithelium with keratin debris. In addition, imaging modalities such as contrast-enhanced CT scan, skin and soft tissue ultrasonography, or MRI can be used to visualize the lesion and measure its extent. 9
On histopathological examination, the lining of branchial cysts is generally lined with squamous epithelium but sometimes pseudostratified, columnar and ciliated. The lining may be ulcerated. The connective tissue wall contains abundant lymphoid tissue, indicating germinal centers. 7
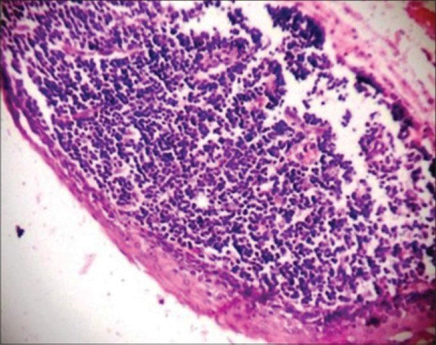
Picture 2.5 A patient woman aged 50 year come to RS with complaint of swelling in the lower jaw since 4-5 months. Photomicrograph shows cystic lumen lined by thin stratified squamous epithelium with flat rete ridges and underlying connective tissue showing abundant lymphoid tissue aggregates (H&E stain, ×100). 7
Treatment
Treatment of branchial cleft cysts is elective excision because the risk of infection, further enlargement, or malignancy is very low. As long as there is no obstruction airway or abscess that Clearly, there is usually no urgency; the doctor may delay excision beyond 3 to 6 months of age or allow treatment of acute infection. However, if there is airway compromise or a large abscess, emergency surgery is needed. may be necessary. 14 Systemic antibiotics and aspiration is generally preferred over incision and drainage, which may result in more distortion of the surgical field. 17
The incision is planned to optimize cosmetics, placing it in folds skin experience If possible. If there is fistula or sine, therefore identifying the tract by carefully inserting a probe or catheter is important to ensure complete excision and reduce the chance of recurrence. Methylene blue can used with dip probe lacrimal into the solution and insert it into the canal to make it easier to identify intraoperatively. Dissection should be done carefully on the surface of the lesion because the canal can be thin-walled. If the path is long, then Exposure must obtained with use incision "stepladder" second which is placed in a skin crease cephalad to the main incision. In the first branchial cleft cyst, initial exposure of the main trunk of the facial nerve and its branches should be performed with a superficial parotidectomy approach to reduce the risk of facial nerve injury, as the anomaly may be closely associated with the nerve. Fistulogram pre operation Also can useful. 18 If patient No can undergoing surgery, ethanol ablation has been used as an alternative in this patient population, although it is not usually recommended as primary treatment. 19
The third and fourth branchial cleft cysts were treated with a transverse cervical incision. standard For identify nerve laryngeal repetitive, sometimes requires a thyroid lobectomy to completely bypass the tract to the pyriform sinus. Before the transcervical portion of the surgery begins, direct laryngoscopy is performed to confirm the diagnosis and allow endoscopic cannulation of the opening into the pyriform sinus to facilitate dissection during excision. 20,21
Complications And Prognosis
Once a branchial cleft cyst has been removed, recurrence is relatively rare. There is an estimated risk of 3%. However, if previous surgery or recurrent infection has happen, relapse Can reach 20%. Patient And family must It is well known that branchial cleft cysts are usually benign, and with treatment, patients generally recover without complications or recurrence. 7,16
Branchial cleft anomalies are congenital malformations, and currently, there are no preventive measures to reduce the likelihood of their occurrence. Patients and physicians should be educated about the symptoms and physical examination findings that may lead to early diagnosis of these lesions. This may reduce the cost of care for the patient, which would otherwise consist of future physician visits, multiple antibiotic courses, and diagnostic imaging. 16
REFERENCE
Just do it AE, Adeoye HE. Prevalence, risk factors and outcome of congenital anomalies among neonatal admissions in OGBOMOSO, Nigeria. BMC Pediatr. 2019 Apr 3;19(1).
Chimah OU, Emeagui KN, Ajaegbu OC, Anazor C V., Ossai CA, Fagbemi AJ, et al. Congenital malformations: Prevalence and characteristics of newborn admitted into Federal Medical Center, Asaba. Health Sci Rep. 2022 May 1;5(3).
Sarkar S, Patra C, Dasgupta MK, Nayek K, Karmakar PR. Prevalence of Congenital Anomalies in Neonates and Associated Risk Factors in a Tertiary Care Hospital in Eastern India. J Clin Neonatol. 2013;2(3):131.
Lean SC, Derricott H, Jones RL, Heazell AEP. Advanced mother age and adverse pregnancy outcomes: A systematic review and meta-analysis. PLoS One. 2017 Oct 1;12(10).
Ekwunife Oh, Okoli C, Ugwu J, Modekwe V, The Ecwesia A. Congenital anomalies: Prospective study of patterns and associated risk factors in infants presenting to a tertiary hospital in Anambra State, South-east Nigeria. Niger J Paediatr. 2017 Jan 1;44(2):76–80.
Adams A, Mankad K, Offiah C, Childs L. Branchial cleft anomalies: a pictorial review of embryological development and spectrum of imaging findings. Imaging Insights. 2016 Feb 1;7(1):69–76.
Chavan S, Deshmukh R, Karande P, Ingale Y. Branchial cleft cyst: A case report and review of literature. J Oral Maxillofac Pathol. 2014;18(1):150.
Magdy EA, Fadali GA, Seif-Elnasr M, Fathalla MF. Unusual Isolated Parapharyngeal Second Branchial Cleft Cyst: A Case Report and Literature Review. Case Rep. Otolaryngol. 2020 Dec 8;2020:1–7.
Hamadi IS, Lutfi L, Mohammed AA, Alkhadem Z. Branchial Cyst in the Parapharyngeal Space: A Case Report. Dubai Medical Journal. 2021 Jul 1;4(2):171–4.
Long KL, Spears C, Kenady DE. Branchial cleft cyst encircling the hypoglossal nerve. J Surg Case Rep. 2013 Sep 1;2013(9):rjt068–rjt068.
Meng F, Zhu Z, Ord RA, Zhang T. A unique location of branchial cleft cyst: case report and review of the literature. Int J Oral Maxillofac Surg. 2019 Jun 1;48(6):712–5.
Bahakim A, Francois M, Abbeele T Van Den. Congenital Midline Cervical Cleft and W-Plasty: Our Experience. Int J Otolaryngol. 2018 Dec 2;2018:1–5.
Prosser JD, Myer IM. Branchial cleft anomalies and thymic cysts. Otolaryngol Clin North Am. 2015;48(1):1–14.
Koch EM, Fazel A, Hoffmann M. Cystic masses of the lateral neck - Proposition of an algorithm for increased treatment efficiency. J Craniomaxillofac Surg. 2018 Sep 1;46(9):1664–8.
Tazegul G, Bozoǧlan H, Prayer Oh, Sari R, Altunbas H, Balcy M. Cystic lateral neck mass: Thyroid carcinoma metastasis to branchial cleft cyst. J Cancer Res Ther. 2018 Oct 1;14(6):1437–8.
Coste AH, Lofgren DH, Shermetaro C. Branchial Cleft Cyst. Indian J Dermatol. 2023 Apr 10;61(6):701.
Prada LR, Koripalli VS, Merino CL, Fulger I. A Case of a Rapidly Enlarging Neck Mass with Airway Compromise. J Clin Diagn Res. 2017 May 1;11(5):OD14.
Mattioni J, Azari S, Hoover T, Weaver D, Chennupati SK. A cross-sectional evaluation of outcomes of pediatric branchial cleft cyst excision. Int J Pediatr Otorhinolaryngol. 2019 Apr 1;119:171–6.
Ha EJ, Baek SM, Baek JH, Shin SY, Han M, Kim CH. Efficacy and Safety of Ethanol Ablation for Branchial Cleft Cysts. AJNR Am J Neuroradiol. 2017 Dec 1;38(12):2351.
Ahn D, Lee GJ, Sohn JH. Comparison of the Retroauricular Approach and Transcervical Approach for Excision of a Second Brachial Cleft Cyst. J Oral Maxillofac Surg. 2017 Jun 1;75(6):1209–15.
Teng SE, Paul BC, Bruh JD, Fritz M, Fang Y, Myssiorek D. Endoscope-assisted approach to excision of branchial cleft cysts. Laryngoscope. 2016 Jun 1;126(6):1339–42.
Comments