LITERATURE REVIEW
I Made Nudi Arthana
Cholesteatoma
1 Definition
Cholesteatoma is an abnormality of keratinized squamous epithelial growth in the middle ear, external auditory canal, mastoid bone, and petrous bone. In general, cholesteatoma can be divided into 2 types, namely: congenital and acquired types . Acquired cholesteatoma is divided into primary and secondary. The primary type is characterized by the presence of an intact tympanic membrane and generally the disorder occurs in the pars flaccid . Meanwhile, in the secondary type, there is perforation of the tympanic membrane and the disorder occurs in the pars tensa . Most cases of cholesteatoma are the acquired type . 1-21
2 Etiology
Until moment This, etiology from cholesteatoma Still Not yet known with clear. However, there are several theories that explain the occurrence of cholesteatoma. Theories This includes: theory epithelial rest , theory invagination, theory epithelial invasion, theory metaplasia squamous, theory hyperplasia cell basal, as well as theory traction mucosa, which shows the course of acquired cholesteatoma disease . 22,23epithelial rest theory is the most widely accepted theory regarding cholesteatoma. This theory states that congenital cholesteatoma is caused by epithelial rests. epithelium Which trapped in gap ear middle. Normally, epithelium the undergoes resorption at 33 weeks of gestation. However, due to impaired absorption during embryogenesis, the epithelium remains and over time proliferates into cholesteatoma. This theory is also supported by the fact that the location of the remaining epithelium is in the anterosuperior quadrant of the middle ear, which is also the most common location for congenital cholesteatoma. 22,23The invagination theory is a theory that is quite widely used to explain the causes of acquired cholesteatoma. Cholesteatoma is said to occur because retraction pars flaccid membrane timpani as consequence from pressure negative on the ear Middle, Which where matter This most widely was initiated consequence dysfunction from eustachian tube ( hydrops ex vacuum theory) . Besides dysfunction tube, pressure negative can also caused by the presence of repeated inflammatory processes. The deeper the retraction pocket followed by the accumulation of keratin, the formation of cholesteatoma occurs. The formation of cholesteatoma causes obstruction of the pocket opening which leads to its spread in the middle ear cavity. 23,24
The theory of epithelial invasion or migration was put forward by Habermann and Bezold in 1888 and 1890. This theory explains that cholesteatoma is formed due to the presence of migration or displacement epithelium squamous keratinized membrane timpani towards the ear middle consequence existence defect perforation on membrane the. Theory This supported by studies on experimental animals that show the presence of medial squamous epithelial displacement through marginal perforations. 24,25
Furthermore, the squamous metaplasia theory explains the formation of cholesteatoma. through process metaplasia on mucosa ear Middle. Process This occurs due to inflammation or infection. Inflammatory or infectious conditions trigger the keratinization process of pluripotent mucosal epithelial cells. This will cause enlargement of the cholesteatoma, resulting in lysis and perforation of the tympanic membrane. This picture is most often found on acquired type cholesteatoma . 24.25
The basal cell hyperplasia theory explains that the formation of cholesteatoma begins with process proliferation keratinocytes cell basal so that to form microcyst Which containing keratin (pseudopodia). Pseudopodia can invade tissue subendothelial Prussak's space , which is a gap bounded by the neck of the malleus medially, the pars flaccida laterally, the lateral malleolus fold superiorly, and the lateral process of the malleus inferiorly. The inflammatory process is thought to be the trigger for tissue proliferation. However, Not yet there is study Which can explain direction growth of basal cells toward the medial direction. This theory is used to explain cholesteatoma in intact tympanic membrane. 24,25
The mucosal traction theory explains that the formation of cholesteatoma is based on existence contact part medial membrane timpani with mucosa surface lateral from auditory ossicles. There is contact between both structures can pull the tympanic membrane superiorly. The pulling can occur due to cilia on the mucosa, mucus, or movement of the epithelial cell layer itself. This process is followed by the formation of proinflammatory elements and cytokines produced by the mucosa, thus triggering keratinocyte proliferation and migration. Cholesteatoma will form through the accumulation of keratin that experiences impaction on the orifice. 253
3 Epidemiology
The true incidence of cholesteatoma worldwide is unknown. Many retrospective studies have been conducted to obtain accurate demographic statistics. A study in the United States reported six cholesteatomas per 100,000 people. The mean age of children diagnosed with acquired cholesteatoma was 9.7 years. Acquired cholesteatoma is about 1.4 times more likely to occur in males than females. A study in the United Kingdom found an increased incidence of cholesteatoma in areas where in a way socioeconomic experience lag, Which where show that the incidence of acquired cholesteatoma is higher in low-income populations, although further research is needed in this area. 20,26 Most cholesteatomas are acquired . Congenital cholesteatoma occurs in 2% of middle ear cholesteatoma patients. Research conducted in Brazil showed that 24.5% of CSOM patients will experience cholesteatoma with an average age of 34.49 years. Most patients are female and have lesions in the right ear. Patients also have a risk of experiencing cholesteatoma on ear contralateral as big as 7% until 20%. Research conducted in Italy also showed more or less similar results. The average age of sufferers was 41.2 years with a predilection for female sufferers. Most sufferers complained of hearing loss and otorrhea. As many as 64.5% sufferer undergo operation canaloplasty as order laksana. 22,23,27,28 There is no data on epidemiology that shows the incidence rate of cholesteatoma nationally in Indonesia. Cholesteatoma can cause an increase mortality, especially on case Which cause the occurrence intracranial complications. Even though thus, mortality consequence cholesteatoma reported very Rarely. However, complications of cholesteatoma can cause permanent deafness. 20
4 Pathophysiology
The process of erosion and bone invasion are important factors related to the pathophysiology of cholesteatoma. As the lesion grows, the presence of cholesteatoma can play a role in damage antrum, process mastoid, as well as structure ear middle other (auditory bones, channel nerve facialist, tag timpani, And wall channel semicircularis). Damage to these structures has the potential to cause disorders in the central nervous system, like abscess brain And meningitis. Process resorption bone started with there is an increase in mononuclear cells in the bone marrow, which is a process that plays a role in increase osteoclast activity. The resorption process Also supported by the increase proinflammatory cytokines as well as existence activation cell T And B. Activation cell T and B will increase the levels of receptor activator of nuclear factor kappa-Β ligand (RANKL), which plays a role in increasing bone resorption activity. Another theory is also show role enzyme collagenase, beta hexosaminidase, nitrogen oxide, and matrix metalloproteinase in the bone destruction process of cholesteatoma patients. 22,26,28
In addition, infection also plays an important role in the pathogenesis and aggressiveness of cholesteatoma. It is proven that bacterial biofilms are commonly formed and found in the middle ear of cholesteatoma patients. Biofilm production occurs due to an imbalance between oxidative and antioxidant processes. on bacteria, especially Pseudomonas aeruginosa, which is a bacteria commonly found in middle ear infections. Biofilm will induce process inflammation chronic as well as proliferation And bone resorption. Existence bacteria, especially Staphylococcus aureus, Proteus sp., Peptococcus sp., And Bacteroides sp. Also can to aggravate process destruction bone. This process occurs through the production of acids that lower the pH of cholesteatoma debris and stimulate the invasive and proliferative properties of the epithelium. 23,25,29
5 Diagnosis
Diagnosis cholesteatoma need suspected on patient with otorrhea Which no pain, often repetitive, or Which No visit healed with treatment. Patient can also complain of conductive deafness, dizziness, or the emergence of symptoms of cranial nerve complications. In congenital cholesteatoma, patients may be asymptomatic and have no history of otorrhea, tympanic membrane perforation, or have had ear procedures. Patients may present with manifestations of complications from cholesteatoma, such as the emergence of neck abscesses or central nervous system disorders due to abscess epidural, meningitis, and sine thrombosis sigmoid. Temporary, patients with cholesteatoma type acquired usually complain about otorrhea smelly Which arise in a chronic although Already Once get antibiotics previously. Giving antibiotics will not stop otorrhea. This is because there is no blood supply. blood on cholesteatoma, so that giving antibiotics difficult eradicate the infection condition. Patients can also come with complaints of hearing loss or even deafness. This occurs due to the filling of the middle ear cavity by desquamated epithelium or damage to the auditory ossicles. The presence of a labyrinthine fistula or the location of cholesteatoma that occurs close to the stapes bone can cause complaints of dizziness and balance disorders. Other non-specific complaints, such as fever, nausea, vomiting, and facial nerve disorders can also occur. The presence of otalgia or dull ear pain can occur, but is rare. This symptom occurs in acute exacerbation conditions and is often associated with intracranial spread. 25,30
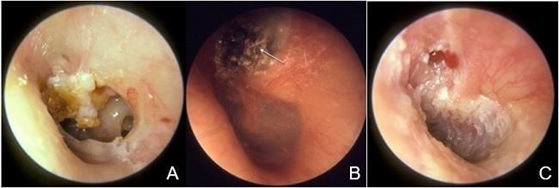
On physical examination, there will be drainage or granulation tissue in the ear canal and middle ear. Otoscopic examination will also show changes in the external acoustic meatus, such as edema, otorrhea, and may be accompanied by perforation of the tympanic membrane. The picture of acquired cholesteatoma is shown in Figure 1. In patients with congenital type, membrane timpani Still still intact And found existence mass pearly white in the antero-superior quadrant of the tympanic membrane. This image can be seen in Figure 2. Using a microscope may also be helpful. A collection of white keratin flakes can often be seen in the posterosuperior quadrant of the tympanic membrane. 25,30,31
Tuning fork examination can also be performed to assess the function and determine the type of hearing loss experienced. Patients may experience conductive hearing loss as a result of damage to the auditory ossicles. In more severe conditions, damage to the intratemporal structure can cause sensorineural hearing loss. Assessment of facial nerve function and palpation of the temporomandibular joint are also important to determine the extent of the cholesteatoma lesion experienced by the patient. 25,31
The presence of cholesteatoma also needs to be confirmed through radiological examination. Computed tomography (CT) scan is used to help confirm lesi cholesteatoma And disturbance on bone temporal. Besides Therefore, CT scan can help determine the location of cholesteatoma, identify complications, and assess the presence/absence of bone erosion. Typical features that can be found are the presence of well-defined soft tissue lesions that are expansive, tympanic membrane retraction, blunting of the scutum, and erosion of the tegmen tympani and ossicles. 31,32 Furthermore, magnetic resonance imaging (MRI) examination is also one of the supporting examination options that can be used to confirm the diagnosis of cholesteatoma, especially if the clinical findings are doubtful. MRI examination can differentiate cholesteatoma from conditions such as fibrosis, network granulation, granuloma cholesterol, and process inflammation. MRI image type signal intensity usually No give description Which typical. Generally, lesions are shown as hypointensity or isointensity on T1W1 and hyperintensity on T2W1 compared to brain tissue. The diffusion-weighted MRI examination type has been reported to have high sensitivity, specificity, and positive and negative predictive values in establishing the diagnosis of cholesteatoma. MRI type BI give description improvement intensity related with effect diffusion and effect shine through T2. Study latest show artifact Which more minimal and better contrast was found on DWI-PROPELLER examination.31,32
Audiometry examination is usually performed to assess the patient's hearing function. cholesteatoma And confirm findings inspection physique. Part big Cholesteatoma patients will experience mixed-type hearing loss. Cholesteatoma located in the external acoustic meatus will show a conductive type of hearing loss. Sensorineural hearing loss occurs when the internal auditory canal is involved. Total hearing loss is rare. However, if it occurs, it is due to a labyrinthine fistula that causes labyrinthitis. Audiometry examination should always be performed before surgery to determine baseline values. The thresholds for sound reception, air conduction, and bone conduction, as well as speech discrimination scores should be recorded. 20,31,32
Picture 2.2 Description cholesteatoma type acquire
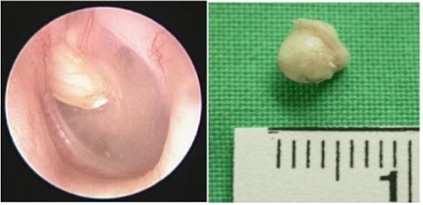
Picture 2.3 Description cholesteatoma type congenital. 31
6 Treatment
The management of cholesteatoma is eradication of cholesteatoma with surgery. The choice of surgery is based on the spread of cholesteatoma and the condition of the tympanic membrane and ossicles. Patients often come with disturbing pain and hearing loss. It is important to explain that the goal of surgery is to remove the cholesteatoma, which cannot restore the patient's hearing to normal. In fact, the patient's hearing may decrease after surgery, so it is important to discuss this possibility with the patient. 20,27
In general, mastoidectomy surgery can be divided into 2 techniques, namely: canal-wall-up (CWU) and canal-wall-down (CWD). The principle of the CWU procedure is to eliminate all mastoid cells and maintain the posterior auditory canal wall. The CWU procedure has a faster healing rate and does not require cleaning routine in channel ear outside. Patient incidence Which Residual cholesteatoma is more common in CWU due to limited surgical access to assess the middle ear cleft. In the CWD procedure, the wall posterior channel auditory lifted part, so that hole ear And mastoid into one unit. This technique allows for better visualization of the middle ear. Better visualization will make it easier to detect recurrences, reduce earwax, and the risk of recurrent infections accompanied by otorrhea. The disadvantages of this procedure are that the patient will need aural toilet for life, vertigo can occur when stimulated by water in the ear canal, a longer healing process, poor cosmetic appearance, and difficulty using hearing aids. Mastoidectomy can be performed through approach in a way microscopic And endoscopy. Approach microscopic done through endural or post auricle. Use endoscopy moment This have more Lots profit Because give visualization more Good And minimize intraoperative incisions.21,33,34
Mastoid obliteration is performed together with the CWD technique, which aims to reduce otorrhea, recurrence, and infection related to the size of the gap in the mastoid. Closure of the mastoid cavity can be done using biological graft materials , such as bone, fascia, and cartilage, or non-biological grafts, such as calcium phosphate. and hydroxyapatite. The secondary purpose of surgery in cholesteatoma patients is to create a dry ear situation and restore mechanism transfer voice, so that repair hearing patients. The surgical techniques performed are tympanoplasty and ossiculoplasty. Ossiculoplasty uses materials such as bone or cartilage grafts , or synthetic prostheses, For replace bone hearing Which experience damage. However, the evidence show that as much as 5-50% operation No succeed And resulting in relapse. 20,35,36
7 Prognosis And Complications
In most cases, cholesteatoma can be removed, but often requires multiple operations. Currently, complications from cholesteatoma are rare. Reoperation is performed in only 5% of patients with the CWD tympanomastoidectomy technique. The CWU technique is associated with a much higher recurrence rate. However, hearing loss is often permanent. Death from cholesteatoma is very rare today. Complications of cholesteatoma Which often found is fistula labyrinth. Fistula labyrinth marked by disturbance auditory And vestibular. Condition This was initiated by erosion bone endochondral in the labyrinthine part which functions to protect the endosteum, perilymph, and endolymphatic compartments from pressure or mass-related movements. 20
CT Scan Temporal
Computed Tomography (CT) Scan is the main choice in diagnosis and in assessing the extent and complications caused by CSOM. In patients with CSOM, through CT Scan we can see decreased pneumatization of the mastoid air cells and sclerotic changes in the mastoid bone. Opacification of the air cells will be seen. These findings are secondary to chronic inflammation and recurrent infections. 10,11,12
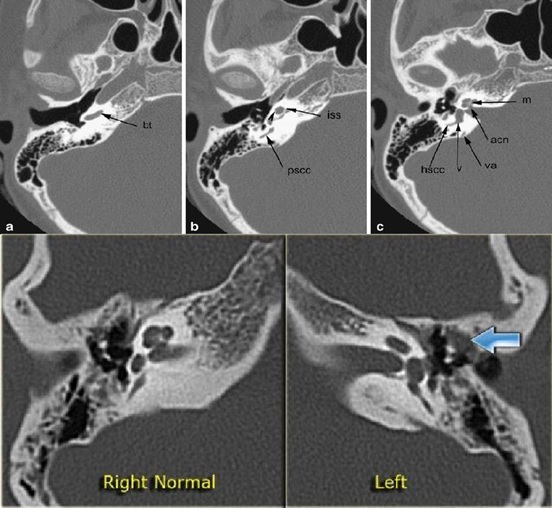
Picture 2.4 CT Scan Temporal
Cholesteatoma is an accumulation of keratin originating from the migration of epithelium. squamous. On CT Scan will looks as soft tissue mass on middle ear accompanied by erosion or destruction of the ossicles, scutum, lateral walls epitympanum, canal semicircular lateral And tag tympanic. CT scan of cholesteatoma will show bone demineralization, erosion and destruction in addition to findings of chronic otitis media. The ossicles are medial displacement by cholesteatoma in the pars flacida or lateral displacement in the pars tensa. Without bone destruction, it is difficult to differentiate from simple granulation tissue or fluid associated with chronic otitis media. 10,11,12
Acquired cholesteatoma most commonly occurs in the pars flacida of the tympanic membrane and forms a mass in the prussak's space which is the space between the ossicles and the lateral wall of the epitympanum. Erosion of the scutum, the lateral wall of the epitympanum, and the ossicles are typical findings. Medial displacement of the ossicles may be an early sign of cholesteatoma. Occasionally adhesions to the pars tensa membrane timpani to promoter cochlea produce cholesteatoma formation near the fascial recess in the posterior tympanic cavity. 9,10
REFERENCE
Khadkekar MS, Shinde VS, Shetti MV. Otitis media in children: Prevalence, clinical profile and risk factors in rural India. Int J Curr Med Sci. 2022;8(10):546- 50.
Tamilarasan V, Parameswari V, Chandrasekaran K. Risk factors and microbial profile in chronic otitis media. J Otolaryngol Res. 2022;9(4):235-41.
Akhtar M, Sheikh MA. Analyzing cholesteatoma-related complications in chronic otitis media. Asian J Med Health Sci. 2020;12(6):411-7.
Haque M, Hasan MJ, Miah MR. Complications of chronic suppurative otitis media: A review. Int J Clin Med Sci Res. 2023;5(3):64-72.
Patil S, Harshitha MC, Girish PB. Clinical profile of chronic suppurative otitis media (CSOM) patients. J Cardiovasc Dis Res. 2023;14(6):1770-1.
Moruskar A, Karodpati N, Ingale M, Shah S. Study of pattern of hearing loss in CSOM (chronic suppurative otitis media). Trop J Ophthalmol Otolaryngol. 2019;4(2):131-9.
Christianty S, Wahyudiono M. Patterns of ear disease in ENT clinic, Indonesia. Indonesian J Med. 2020;10(3):98-104.
Cetinkaya EA, Topsakal V. Acute Otitis Media. Pediatr ENT Infect [Internet]. 2023 Apr 15 [cited 2023 Dec 19];381–92. Available from : https://www.ncbi.nlm.nih.gov/books/NBK470332
Rosary DC, Mendez MD. Chronic Suppurative Otitis. StatPearls [Internet]. 2023 Jan 31 [cited 2023 Dec 19]; Available from : https://www.ncbi.nlm.nih.gov/books/NBK554592
Poluan FH, Utomo BSR, Dharmayanti J. PROFILE BENIGN TYPE OF CHRONIC SUPPURATIVE OTITISMEDIA IN GENERAL HOSPITAL OF THE CHRISTIAN UNIVERSITYOF INDONESIA. Int J Res - GRANTHAALAYAH [Internet]. 2021 May 1 [cited 2023 Dec 19];9(4):229–39.Available from: https:// www.granthaalayahpublication.org/journals/ind ex.php/Granthaalayah/
Hidayat R. Pathophysiological to Clinical Aspects of Chronic Suppurative Otitis Media (CSOM): Narrative Literature Review. Arch Med Case Reports [Internet]. [cited 2023 Dec 19];3:2022. Available from: https://hmpublisher.com/index.php/AMCR/article/view/175
Otitis Media: Practice Essentials, Background, Pathophysiology [Internet]. [cited 2023 Dec 19]. Available from:
Özcan N, Saat N, Baylan MY, Med NA-I, 2018 U. Three cases of Chronic Suppurative Otitis Media (CSOM) caused by Kerstersia gyiorum and a review of the literature. K GülInfez Med [Internet]. 2018 [cited 2023 Dec 19]; Available from: https: //www.a c ademia.edu/download/79013211/Vol_26_4_2018_11.pdf
Binti F, Alkatiri B. CRITERIA DIAGNOSIS AND IMPLEMENTATION
OTITIS MEDIA SUPPURATIVE CHRONIC. Essence Science Medical [Internet]. 2016 Apr
15 [cited 2023 Dec 19];5(1):100–5. Available from: https://mail2.isainsmedis.id/index.php/ism/arti cle/view/42
Chronic Suppurative Otitis Media: Practice Essentials, Anatomy, Pathophysiology [Internet]. [cited 2023 Dec 19]. Available from: https://emedicine.medscape.com/article/859501-overview
Paul Flint, Bruce Haughey, Valerie Lund, K. Robbins, J. Regan Thomas, Marci Lesperance, et a. CUMMINGS Otolaryngology - INTERNATIONAL
EDITION : head and neck surgery. 2020 [cited 2023 Dec 19];7:1323–44. Available from: https:// www.worldcat.org/title/1239324944
Jackler RK, Santa Maria PL, Varsak YK, Nguyen A, Blevins NH. A new theory on the pathogenesis of acquired cholesteatoma: Mucosal traction. Laryngoscope [Internet]. 2015 Aug 1 [cited 2023 Dec 20];125(S4):S1–14. Available from: https://onlinelibrary.wiley.com/doi/full/10.1002/lary.25261
Health science textbook : ear nose throat head & neck. 2012 [cited 2023 Dec 19]; Available from: https://lib.ui.ac.id
Uddene F, Philip M, Reimer A, Paul M, Matuschek E, Thegerstrom J, et a. Aerobic bacteria associated with chronic suppurative otitis media in Angola. Infect Dis Poverty [Internet]. 2018 May 3 [cited 2023 Dec 19];7(1):1–10. Available from: https://li nk.springer.com/articles/10.1186/s40249-018-0422-7
Kennedy KL, Singh AK. Middle Ear Cholesteatoma. StatPearls [Internet]. 2023 Jul 4 [cited 2023 Dec 19]; Available from: https: //www.ncbi.nlm.n ih.gov/books/NBK448108/
Volgger V, Lindeskog G, … EK-BJ of, 2020 U. Identification of risk factors for residual cholesteatoma in children and adults: a retrospective study on 110 cases of revision surgery. Brazzers J Otorhinolaryngol [Internet]. 2020 [cited 2023 Dec 19];
Available from : https://www.scielo.br/j/bjorl/a/hYd4CspcYHq7By8xvrp8pWv/?lang= e n
Kansu L, Ozluoglu LN. Congenital cholesteatoma together with ossicular chain anomaly. Eur Arch Oto-Rhino-Laryngology. 2017 Feb 1;274(2):1179–82.
Kuo C, Shiao A, Wen H, Laryngoscope WC-T, 2018 U. Increased risk of cholesteatoma among patients with allergic rhinitis: A nationwide investigation. Laryngoscope [Internet]. 2018 Mar 1 [cited 2023 Dec 19];128(3):547–53. Available from: https://onlinelibrary.wiley.com/doi/abs/10.1002/la ry.26220
Kuo CL. Etiopathogenesis of acquired cholesteatoma: Prominent theories and recent advances in biomolecular research. Laryngoscope. 2015 Jan 1;125(1):234– 40.
Jackler RK, Santa Maria PL, Varsak YK, Nguyen A, Blevins NH. A new theory on the pathogenesis of acquired cholesteatoma: Mucosal traction. Laryngoscope [Internet]. 2015 Aug 1 [cited 2023 Dec 20];125(S4):S1–14. Available from: https://onlinelibrary.wiley.com/doi/full/10.1002/lary.25261
Khalid-King M, Tikka T, Coulson C. Cholesteatoma: a disease of the poor (socially deprived)? Eur Arch Oto-Rhino-Laryngology. 2015 Oct 24;272(10):2799–805.
Medany M, Sabra R, … EH-… EJ of, 2018 undefined. Reliability of Diffusion Weighted MRI for the Diagnosis of Residual and Recurrent Cholesteatoma. ejhm.journals.ekb.egMM Medany, RM Sabra, EK Hakim, AMM Elshafei, AMI SadawyThe Egyptian J Hosp Med 2018•ejhm.journals.ekb.eg [Internet]. [cited 2023 Dec 20]; Available from: https://ejhm.journals.ekb.eg/a rticle_11297.html
Udayabhanu HN, Prasad SC, Russo A, Greenblade G, Sanna M. Cholesteatoma of the external auditory canal: Review of staging and surgical strategies. Otol Neurotol [Internet]. 2018 [cited 2023 Dec 20];39(10):e1026–33. Available from: https://journals.lww.com/otologyneurotology/fulltext/2018/12000/cholestea toma_of_the_external_auditory_can
Hamed MA, Nakata S, Sayed RH, Ueda H, Badawy BS, Nishimura Y, et al. Pathogenesis and Bone Resorption in Acquired Cholesteatoma: Current Knowledge and Future Prospectives. Clin Exp Otorhinolaryngol [Internet]. 2016 Dec 1 [cited 2023 Dec 20];9(4):298–308. Available from: https://synapse.koreamed.org/articles/1157604
Cholesteatoma: Practice Essentials, Background, Etiology and Pathophysiology [Internet]. [cited 2023 Dec 20]. Available from: https://emedicine.medscape.com/article/860080-overview
Emmett SD, Kokesh J, Kaylie D. Chronic Ear Disease. Med Clin North Am [Internet]. 2018 Nov 1 [cited 2023 Dec 20];102(6):1063–79. Available from: http://www.medical.theclinics.com/article/S0025712518300683/fulltext
Baráth K, Huber AM, Stämpfli P, Varga Z, Kollias S. Neuroradiology of Cholesteatomas. Am J Neuroradiol [Internet]. 2011 Feb 1 [cited 2023 Dec 20];32(2):221–9. Available from: https:// www.ajnr.org/content/32/2/221
Bae MR, Kang WS, Chung JW. Comparison of the Clinical Results of Attic Cholesteatoma Treatment: Endoscopic Versus Microscopic Ear Surgery. Clin Exp Otorhinolaryngol [Internet]. 2018 May 1 [cited 2023 Dec 20];12(2):156– 62. Available from: https://synapse.koreamed.org/articles/1157732
Kuo CL, Shiao AS, Yung M, Sakagami M, Sudhoff H, Wang CH, et al. Updates and knowledge gaps in cholesteatoma research. Biomed Res Int. 2015;2015.
Ghiasi S. Mastoid Cavity Obliteration with Combined Palva Flapand Bone Pâté. Iran J Otorhinolaryngol [Internet]. 2015 [cited 2023 Dec 20];27(78):23. Available from: /pmc/articles/PMC4344971/
Quaranta N, Taliente S, Coppola F, Salonna I. Cartilage ossiculoplasty in cholesteatoma surgery: hearing results and prognostic factors. Acta Otorhinolaryngol Ital [Internet]. 2015 Oct 1 [cited 2023 Dec 20];35(5):338. Available from: /pmc/articles/PMC4720926/
Comments