TOTAL MAXILLECTOMY WITH APPROACH WEBER FERGUSON WITH LYNCH MODIFICATION IN CASE OF SINONASAL SQUAMOUS CELL CARCINOMA
I Made Nudi Arthana
Maxillectomy is a surgical procedure for sinonasal carcinoma with the principle of action being resection and removal. Maxillectomy is surgery Which Lots done in stage III or IV sinonasal carcinoma. The Weber Ferguson approach with Lynch modification in this case was performed to expand access to the skull base considering the extent of the tumor.
LITERATURE REVIEW
Carcinoma Sinonasal
Anatomy Nose And Sine Paranasal
The nose is the most prominent part of the face. Anatomically, it is divided into the outer nose or nasal pyramid and the nasal cavity or nasal cavity. The structure of the outer nose from top to bottom consists of the base of the nose ( nose bridge ), nasal bridge or dorsum nasi, tip of the nose , ala nasi, columella And hole nose or nares anterior. Nose outside coated by a framework of bones and cartilage covered by skin, connective tissue and some small muscles For to widen or narrow down hole nose. Framework bone consist of bone nose ( os nasal ), process frontalis bone maxilla And process nasalis frontal bone. The cartilaginous framework consists of several cartilages, namely a pair of superior lateral nasal cartilages, a pair of inferior lateral nasal cartilages. Which also called as cartilage alarm major, a number of install the minor alar cartilages and the anterior edge of the septal cartilages. 5,6
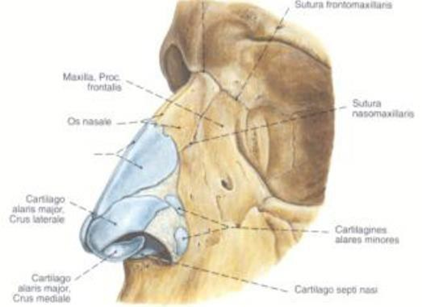
Picture 2.1 Frame Nose, Lateral View . 5
Cavity nose or cavity rice right And left separated by septum the rice in the middle. The front entrance is called the anterior nares and the back is called the posterior nares or choana which connects the nasal cavity to the nasopharynx. Each nasal cavity has 4 walls, namely the medial wall, lateral, inferior And posterior. Wall medial consists of from septum rice. On the lateral wall there are 4 conchae, namely the inferior conchae, the middle conchae, the superior conchae and the supraconchae (usually rudimentary). Between the conchae and the wall lateral there is cavity narrow Which called meatus. Meatus inferior located between the inferior concha and the base of the nose, there is the opening of the nasolacrimal duct. The middle meatus is located between the inferior and middle concha. In the middle meatus there are openings of the frontal, maxillary and anterior ethmoidal sinuses. The superior meatus is the space between the middle and superior concha. In this meatus the posterior ethmoidal and sphenoidal sinuses open. 5,6
The nasal septum is a partition that divides the nasal cavity into two nasal cavities and is anatomically formed by bone and cartilage structures. The bone parts are the perpendicular lamina of the ethmoid bone, the vomer, the nasal crest of the maxillary bone and the nasal crest of the palatine bone. While the cartilage part is cartilage septum, laminate quadrangular And columella. Septum coated by the perichondrium on the cartilage part and the periosteum on the bone part, while on the outside it is lined by the nasal mucosa. 5,6
The vascularization of the nose comes from the internal carotid artery and external carotid artery which supply blood to the nasal septum and lateral wall of the nose. The external nose receives blood supply from the facial artery which is derived from the external carotid artery and the ophthalmic artery which is derived from the internal carotid artery. The internal nose receives blood from the internal carotid artery and external carotid artery. The ophthalmic artery branches into the anterior and posterior ethmoidal arteries, entering the nasal cavity. The anterior ethmoidal artery supplies the anterior septum and lateral wall of the nose. The posterior ethmoidal artery supplies the posterior septum and lateral wall of the nose. Internal maxillary artery Which originate from artery carotid external branching become artery sphenopalatine and greater palatine arteries. The sphenopalatine artery enters the nasal cavity through the sphenopalatine foramen located lateral to the posterior end of the middle concha. In the nasal cavity the sphenopalatine artery branches into artery nasal lateral Which supply blood wall lateral nose And posterior nasal septal artery that supplies the nasal septum. The external carotid artery also branches into the facial artery and then into the superior labial artery. 5,6
On part front septum rice there is anastomosis from branch- arterial branch sphenopalatine, artery ethmoidalis anterior, artery labial superior, artery palatine major called Keisselbach's plexus ( Little area ). Because of its superficial location and easy to be injured by trauma, it becomes a source of nosebleeds. (Warmald, 2006). In the posterior part of the middle concha there is an anastomosis of the sphenopalatine artery and the ascending pharyngeal artery ( Woodruff's area ). This area often causes posterior epistaxis. The veins of the nose have the same name and run together with the arteries. The veins in the vestibule and the outer structures of the nose drain into the ophthalmic vein which is connected to the cavernous sinus. Veins in nose No have valve so that facilitate the spread of infection to the intracranial. 5,6
Nerves part front And superior nose innervated by The anterior and posterior ethmoidal nerves are branches of the nasociliary nerve which originates from the ophthalmic nerve. The rest of the nasal cavity receives most of its sensory innervation from the maxillary nerve via the sphenopalatine ganglion. The sphenopalatine ganglion also provides motor innervation to the nasal mucosa. This ganglion receives sensory fibers from the maxillary nerve, parasympathetic fibers from the greater superficial petrosal nerve and sympathetic fibers from the deep petrosal nerve. Lymphatic drainage from vestibule rice flow to front to direction lips And nose part outside. Flow lymph from fossa nasal flow to posterior Then to area retropharyngeal or subdigastric lymph nodes. 5,6
Histologically and functionally, there are two nasal mucosae, namely the respiratory and olfactory mucosae. The respiratory mucosa is found in most of the nasal cavity and its surface is lined by ciliated pseudostratified columnar epithelium. And in among others there is cell goblet. Mucosa smell there is on roof cavity nose, concha superior And one third on septum. Mucosa This coated by epithelium piston layered pseudo No ciliated And formed by three type cell that is supporting cells, basal cells and olfactory receptor cells. 5,6
There are four pairs of paranasal sinuses in the human body, namely the maxillary sinus, frontal sinus, ethmoid sinus and sphenoid sinus. The sinus cavity is lined by mucosa which is a continuation of the nasal mucosa but is thinner and has fewer glands. The development of the paranasal sinuses begins in the fetus aged 3-4 months except for the frontal sinus and sphenoid sinus, in the form of invagination of the mucosa cavity nose. Sine maxilla And sine ethmoid has There is on time child born. 7
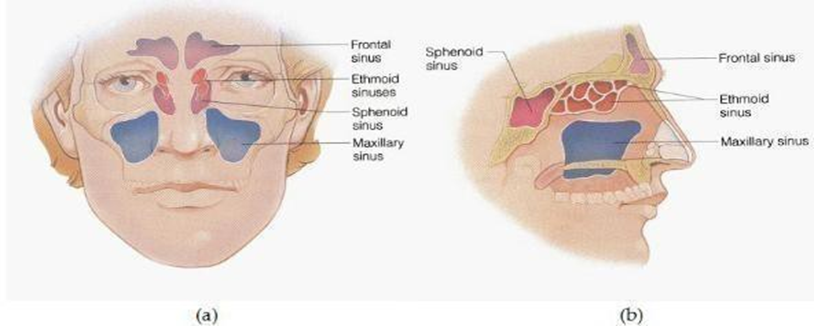
Picture 2.3 Sine Paranasal seen from (a) front and (b) side. 7
Clinically, the paranasal sinuses are divided into two groups, namely the anterior and posterior sinus groups. The anterior group consists of the frontal sinus, maxillary sinus and anterior ethmoid sinus. The posterior group consists of the sphenoid sinus and posterior ethmoid sinus which drain into the superior meatus. The frontal sinus begins to develop from the anterior ethmoid sinus at approximately 8 years of age and will reach its maximum size before the age of 20 years. The frontal sinus drains through its ostium located in the frontal recess. The frontal recess is part of sine ethmoid anterior. Sine sphenoid located in OS sphenoid in behind ethmoid sinus posterior. Pneumatization sine sphenoid started on age 8-10 year. The ostium of the sphenoid sinus leads to the sphenoethmoid recess. These sinuses generally reach their maximum size between the ages of 15-18 years. The optic nerve, carotid artery and cavernous sinus are very close to these sinuses. 7
The maxillary sinus is pyramidal in shape. The anterior wall is the facial surface of the maxillary bone called the canine fossa, the posterior wall is the facial surface infratemporal maxilla, wall medial is wall lateral nasal cavity, the superior wall is the floor of the orbit and the inferior wall is the alveolar process and the palate. The maxillary sinus ostium is located superiorly wall medial sine. Sine maxilla shared become two part by imaginary line Which withdrawn from cantus medial to angle mandible Which called with Ohngren line being the superstructure and infrastructure. Tumors originating from the superior line are associated with a worse prognosis because they are adjacent to the eye, pterygopalatine fossa and infratemporal fossa so that they spread to the cranial fossa and surrounding organs more easily. 7,8
The ethmoid sinuses are hollow cavities consisting of honeycomb-like cells located between the middle concha and the medial wall of the orbit. The ethmoid sinuses are divided into two, namely the anterior ethmoid sinus which empties into the middle meatus and sine ethmoid posterior Which culminate in meatus superior. Cells sine anterior ethmoid usually small-small And Lots whereas cell sine ethmoid posterior bigger And more A little. Side right And left connected by fossa cribriform. Fossa cribriform is Wrong One landmark on determination stadium tumor. Damage to this fossa will cause direct extension of the tumor to the anterior cranial fossa. The lamina papyracea is the lateral wall of the ethmoid that borders the orbit. Damage wall This will cause expansion tumor to orbita. Roof ethmoid formed by fovea ethmoidalis Which is base skull thin . 7.8
Physiology Nose And Sine Paranasal
The three main functions of the nose are smell, respiration, and protection. Some function from sine paranasal between other reduce heavy bone skull because it is considered as an additional space from the nasal cavity that arises due to inadequate ossification, increases voice resonance, moistens and warms the respiratory air so that it can protect internal organs such as the brain from dry and cold air, moistens the nasal cavity and is thought to play a role in the process of smelling, increases fasciocranial resistance to mechanical trauma. 7
Epidemiology
Malignancy sinonasal very seldom found. Malignancy sinonasal only 3% of head and neck malignancies are found and only about 1% of malignancies in all over body. Incident malignancy sinonasal more often happen in Asia and Africa than the United States. Sinonasal malignancies are the second most common malignancies in Asia from head and neck malignancies after carcinoma nasopharynx. 2.4 Period year 2016-2018, in Bali obtained as much as 45 people, the most in the age group 41-60 years, namely 21 patients (46.7%). The most common malignancy in sinonasal is squamous cell carcinoma (70%). The most common predilection in the maxillary sinus (60%), followed by the nasal cavity (20-30%), ethmoid sinus (10-15%), rarely in the frontal and sphenoid sinuses (<1%). Approximately 80% are found at the age of 50-70 years and the incidence in men is twice as frequent as in women. 4.9
Etiology
Etiology carcinoma sinonasal Not yet known Certain, studies epidemiology from various countries show a relationship with exposure to chemicals or industrial materials including nickel, wood dust, leather, furniture, textiles, formaldehyde, chromium, isopropyl oil , and others. Alcohol, cigarette smoke, salted or smoked foods are also suspected of increasing the risk of sinonasal malignancies, especially type carcinoma cell squamous. A number of factor other Which has reported to be the cause, namely agricultural workers, food factories, motor vehicle exhaust fumes And factory textiles. Carcinoma This is disease Which related to the environment. 4.8 The emergence of sinonasal carcinoma is usually not in a short time, but requires long-term exposure and onset up to about 40 years after the first contact and continues after the cessation of exposure. 4.34
Clinical Manifestations
Symptoms depend on the primary origin of the tumor and its direction and extent. Malignant tumors in the maxillary sinus are usually asymptomatic. Symptoms develop after the tumor big, so that urge or penetrate wall bone expand to nasal cavity, oral cavity, cheek, orbit or intracranial. Nasal symptoms include unilateral nasal obstruction and rhinorrhea. The secretions are often mixed with blood or epistaxis occurs. Large tumors can press on the nasal bones, causing nasal deformity. Typically, malignant tumors have a smelly snot because they contain necrotic tissue. Orbital symptoms if there is tumor expansion towards the orbit cause symptoms of diplopia, proptosis (protrusion of the eyeball), ophthalmoplegia, visual disturbances, and epiphora. 10
Oral symptoms may be accompanied by expansion of the tumor into the oral cavity causing protrusion or ulcer in palate or in process alveolar. Patient sigh The dentures are not properly attached or the teeth are loose. Often patients come to the doctor tooth Because painful in tooth, but No healed although tooth Which Sick has been revoked. On patient with symptom facial existence expansion tumor to area face will cause protrusion of the cheeks. Symptoms may be accompanied by pain, loss of sensation (anesthesia or paraesthesia) if it affects the trigeminal nerve. While the extension of the tumor to the intracranial can cause severe headaches, ophthalmoplegia, and visual disturbances. vision, Which can accompanied by liquororrhea, that is fluid brain Which go out through the nose. If the extension reaches the middle cranial fossa, other brain nerves can be affected. caught. If the tumor expand to behind, Trismus occurs due to the pterygoid muscle being affected, accompanied by anesthesia and paresthesia in the area innervated by the maxillary and mandibular nerves. 10,11
Pathophysiology
DNA damage is due in part to its particulate nature, which induces the formation of reactive oxygen species within cells. Several studies have established a causal role for exposure to hardwood dust and textile leather in the development of sinonasal cancers, with a particular association with intestinal-type adenocarcinoma (ITAC) sinonasal carcinoma. 12,15,35
The molecular changes seen in Intestinal-type adenocarcinoma (ITAC) are mainly focused on mutations of TP53, K-ras and H-ras genes and overexpression of EGF or HER2. The K-ras gene was found to be mutated only in cases seldom happen, with report Which contradictory about possibility prognostic role. EGFR and HER2 are overexpressed in approximately 30% of cases. Level mutation TP53 on adenocarcinoma type intestines is around 60% and significantly higher than in squamous cell carcinoma; TP53 mutation rate in ITAC was directly correlated with duration, mean and cumulative level of wood dust exposure. 12,15,35
Diagnosis
Diagnosis is based on anamnesis, physical examination and supporting examinations. Early symptoms may include epistaxis, nasal obstruction, recurrent sinusitis, facial paresthesia, proptosis, diplopia, or asymptomatic mass. in neck. Often, symptoms This copy conditions Which more benign. Patient often ignore symptom- symptom the, or doctor who consider these symptoms as symptoms of infection. When more severe symptoms appear, such as persistent headaches, visual disturbances, the neoplasm has reached an advanced stage and requires complex treatment. It is very important to perform a thorough anamnesis.
It is necessary to ask about hyperesthesia or anesthesia in the cheek area, the presence of masses or inflammation in the facial area, numbness or complaints of loose teeth, dentures that are no longer fixed properly, double vision, difficulty opening the mouth, complaints of a blocked nose, secretions or bleeding, complaints of headaches, disorders of the eye. smell or the exit water eye Keep going continuously. Inspection physique should be performed carefully, with emphasis on the sinonasal region, orbit and cranial nerves, and nasal endoscopy should also be performed. Although not pathognomonic, numbness or hyperesthesia of the infraorbital or supraorbital nerves in a way strong is suspicion invasion malignancy. Findings others like proptosis, chemosis, weakness muscle extraocular, And existence mass in cheek, gingival or gingivo-buccal sulcus are also suspected sinonasal tumors. 12
Supporting examinations that can be performed are radiological examination, endoscopy and biopsy. Radiological examinations such as plain lung photos to see tumor metastasis to the lungs. CT scan examination provides a good picture of the location and extent of the tumor. 15 CT scans can determine the presence of bone erosion or destruction. MRI provides a better picture clear about limit tumor with network soft in surrounding area And help determine expansion tumor to orbit, Dura, brain, a. carotid And sine cavernous. MRI can differentiate tumor masses from secretions or inflamed mucosa. A definitive diagnosis can be made based on histopathological examination. 9,10
Diagnosis of a tumor is based on the histopathology results of a tumor biopsy. Taking biopsy from tumor nose no difficult. Network direct taken with biopsy forceps and the bleeding that occurs is usually managed with anterior packing. Maxillary sinus tumor biopsy is usually performed via the Caldwell-Luc approach, which incises through the gingivo-buccal sulcus. Tumor biopsy sine ethmoid usually taken from expansion tumor in cavity nose or in the middle canthus. Biopsy of the sphenoid sinus tumor was performed via a transnasal approach, but often time biopsy got from expansion tumor to nasopharynx or cavity nose. Biopsy tumor sine frontal done with incision supraorbital and osteotomy. 11,12
Description Histopathological
The most common benign tumor is squamous papilloma followed by inverted papilloma which is very invasive, can damage surrounding tissue and is very... tend For settle down And can changed become malignant. Carcinoma Squamous cells are the most common histopathological picture in sinonasal malignancies (70%), the maxillary sinus is the most frequently affected (65%-80%), followed by the maxillary sinus. ethmoid (15%-25%), whereas sine sphenoid And frontal seldom affected. 13,14
Sinonasal squamous cell carcinoma (SCC) is a malignancy of the head and neck. Which most Lots found, originate from surface mucosa Which lining the aerodigestive tract. In the sinonasal tract, keratinized SCC (KSCC) can occur and non-keratinizing (NKSCC). Subtype verrucosa, basaloid, And spindle Carcinoma is rarely found in the sinonasal cavity. Most sinonasal SCC are KSCC. (60%). In general morphological, KSCC The same with SCC other with stellate, tumor cells with nest Which irregular. Set tumor own Lots cytoplasm eosinophilic containing keratin filaments. Intercellular bridges and keratin production are evident. 25,26
NKSCC (also called Rinertz' carcinoma, transitional cell carcinoma, and Schneiderian carcinoma) is the same type of tumor that occurs in the oropharynx. NKSCC has a " blue cell tumor " appearance that has a high nuclear:cytoplasmic ratio, large, smooth, round bands or nests . with limit Which firm And desmoplasia stroma Which minimum. On Sinonasal SCC has central necrosis and clear mitotic and apoptotic activity. In addition, sinonasal SCC often lines the mucosal surface with undulations, irregular contours, and if it has invaded downwards will give an inverted appearance with round nests (resembling Schneiderian papilloma ). Papillary SCC consists of a thick diffuse tumor with malignant squamous cells. And part big cell to coat papilla And go out to cavity lumens. Basaloid SCC is defined as a basaloid tumor, hyperchromatic cells with round nuclei. Which strung together with lobule And nest shaped round Which each other pressing against each other, divided by a thin line of hyalinized membrane. Spindle cell carcinoma is a pleomorphic or spindled tumor cell with an appearance similar to sarcoma. Spindle cell carcinoma has a picture histology fascicular, collagenose, storiform-plemorphic, And resembles granulation tissue. 25,26
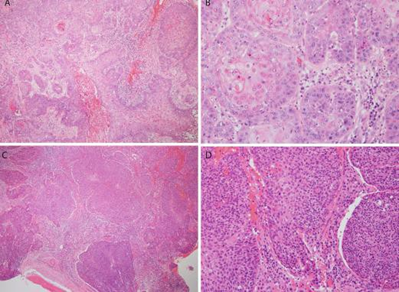
Figure 2.4. KSCC and NKSCC (A: At KSCC with 4x magnification cell view tumor Which big And irregular, And stellate nest on stroma basophilic. B: In KSCC with 20x magnification, cells with abundant eosinophilic cytoplasm and keratinization focus are seen. C: In NKSCC with 4x magnification, large blue cells with minimal stromal reaction and round nests are seen . D: In NKSCC with 40x magnification, hyperchromatic nuclei with minimal cytoplasm and minimal maturation areas of squamous differentiation are seen). 26
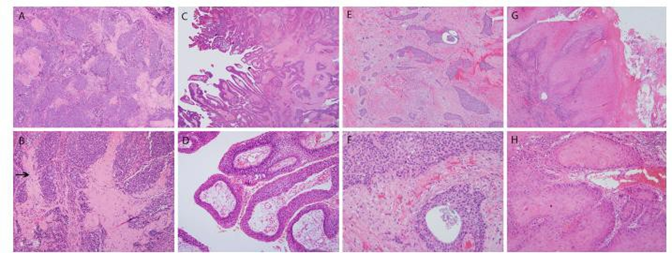
Figure 2.5 Histological variants of SCC (A and B: Basaloid with jigsaw puzzle pattern . C and D: Papillary SCC with dysplastic squamous cells with eosinophilic cytoplasm and hyperchromatic nuclei without maturation. E and F: Carcinoma adenoaquamous Which consists of from SCC with “punched out” glands. F and G: Verrucous carcinoma which is a “hyper-differentiated” tumor with a very thick squamous layer with hyperkeratosis and “ glassy ” with bright eosinophilic cytoplasm, abundant, and pressing the edges without irregular infiltration or stromal reaction). 26
Classification TNM And Stadium
Tumor stage assessment using the American Joint Committee classification on Cancer or AJCC 7th edition year 2018 classify tumor based tumor primary or T, metastasis gland sap clear regional or N and distant metastasis or M. Classification according to AJCC 2018 as follows: 18
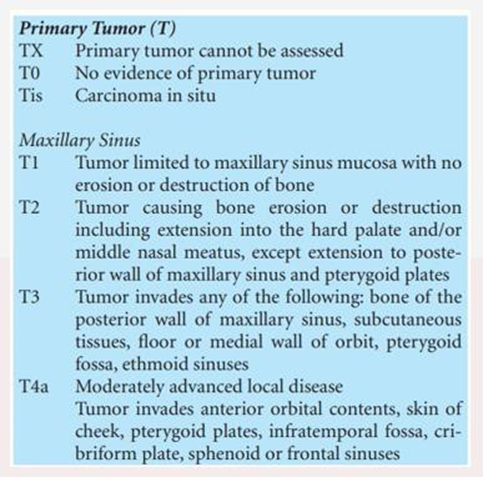
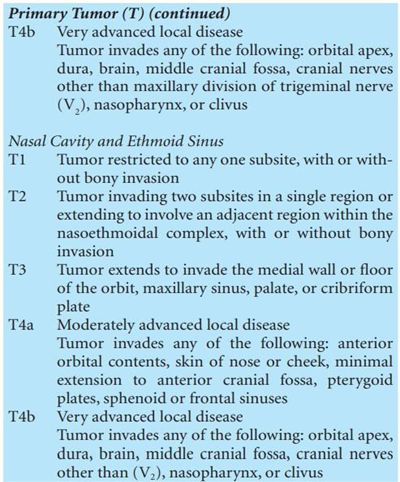
Primary tumor or T is divided into Tx if the primary tumor cannot be assessed. And Tis For carcinoma in there. If tumor primary in sine maxilla then T1 is a tumor limited to the maxillary sinus mucosa, there is no erosion or bone destruction; T2 tumor causes erosion or bone destruction including extension to the hard palate and or middle meatus but there is no extension to the posterior wall of the maxillary sinus and pterygoid fossa; T3 tumor has affected the bone of the posterior wall of the maxillary sinus, subcutaneous tissue, medial wall or floor of the orbit, pterygoid fossa and ethmoid sinus; T4a tumor has affected the anterior orbit, cheek skin, pterygoid plate, infratemporal fossa, cribriform fossa, sine sphenoid or sine frontal; T4b tumor has about apex orbit, dura, brain, middle cranial fossa, cranial nerves other than maxillary or V2, nasopharynx or clivus. 18 If the primary tumor is in the nasal cavity and ethmoid sinus, then T1 is a tumor limited to one side with or without invasion into the bone; T2 the tumor has affected both sides with or without extension into the surrounding tissue. complex nasoethmoid with or without invasion bone; T3 tumor has expand to the medial wall or floor of the orbit, maxillary sinus, palate or cribriform fossa; T4a tumor has about orbit anterior, skin nose or cheek, expansion minimally to the anterior cranial fossa, pterygoid plates, sphenoid sinus or frontal sinus; T4b tumor has involved the orbital apex, dura, brain, middle cranial fossa, cranial nerves other than n. V2, nasopharynx or clivus. 18

Stadium | T | N | M |
0 | Tis | N0 | M0 |
I | T1 | N0 | M0 |
II | T2 | N0 | M0 |
III | T3 | N0 | M0 |
| T1 | N1 | M0 |
| T2 | N1 | M0 |
| T3 | N1 | M0 |
IVA | T4a | N0 | M0 |
| T4a | N1 | M0 |
| T1 | N2 | M0 |
| T2 | N2 | M0 |
| T3 | N2 | M0 |
| T4a | N2 | M0 |
IVB | T4b | Every N | M0 |
| Every T | N3 | M0 |
IVC | Every T | Every N | M1 |
Table 2.7 Tumor Staging (AJCC 7th edition )
Picture 2.6 Classification TNM (AJCC 7th edition )
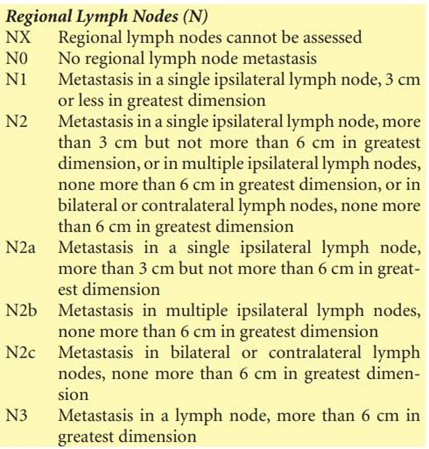
Metastasis to regional lymph nodes or abbreviated N is divided into Nx regional lymph node enlargement cannot be assessed; N0 there is no enlarged lymph node; N1 metastases to lymph nodes single ipsilateral with diameter ≤ 3 cm; N2 metastasis to gland single ipsilateral lymph node more than 3 cm but not more than 6 cm, or multiple ipsilateral ≤ 6 cm or bilateral or contralateral ≤ 6 cm; N2a metastasis to single ipsilateral lymph node more than 3 cm but not more than 6 cm; N2b metastasis to multiple ipsilateral lymph nodes ≤ 6 cm; N2c metastasis to multiple ipsilateral lymph nodes sap clear bilateral or contralateral ≤ 6 cm; N3 metastasis to lymph nodes with a diameter of more than 6 cm. Distant metastasis or abbreviated M is divided into Mx distant metastasis cannot be determined; M0 no distant metastasis; M1 there is distant metastasis. 18
Management
Principle management carcinoma sinonasal is multimodality with surgery as the main option followed by radiotherapy and/or chemotherapy. Election modality This based on to Lots factor between other location, stage, patient condition, comorbidities, facilities (operating room, tools, obturator), operator experience and others. 1,2,14
Maxillectomy is action surgery on carcinoma sinonasal with the principle action is resection And lifting. Action surgery on sinonasal in nature complicated remember his closeness with structure organ vital like eye and the brain. So to get maximum results, cooperation is needed between related multidisciplinary sciences, such as Eye Specialists, Prosthodontists , Surgeons Nerve, And Surgery Plastic Reconstruction specifically on carcinoma advanced sinonasal tumors. There are several types of maxillectomy based on the location, size and extent of the tumor. 1,2,18
Classification Armani
Class I: Resection is performed in the anterior midline of the maxilla, with the abutment teeth on one side of the arch.
Class II: Defect maxillectomy on group This nature unilateral, namely by maintaining the anterior teeth on the contralateral side • Class III: Palatal defects occur in the middle of the hard palate and may involve part of the soft palate.
Class IV: Maxillectomy defect crosses the midline and involves both sides of the maxilla, with abutment teeth present on one side.
Class V: Maxillectomy defects are bilateral and located posterior to the abutment teeth. Labial stabilization may be required.
Class VI: Anterior-anterior upper maxillofacial defect with abutment teeth present bilaterally in the maxillary segment. posterior
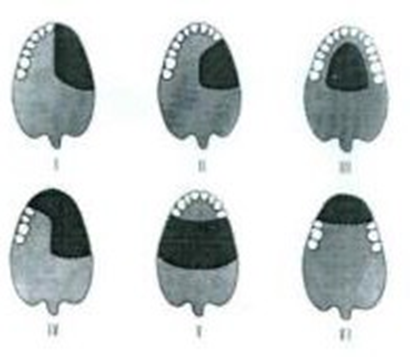
Picture 2.7 Illustration maxillectomy with system Armani
Classification Liverpool
Vertical Components
Class I: Maxillectomy without Oro-Antral Fistula: Removal of alveolar bone Which No produce Fistula Oro-nasal or Oro-antral. Resection sine
ethmoidalis, frontal sinus and/or lateral nasal wall can also be included in this classification.
Class II: Low Maxillectomy: This resection involves the alveolus and antral wall, which will inevitably result in an oro-nasal or oro-antral fistula. The orbital floor or rim remains intact.
Class III: High Maxillectomy: In this category, the orbital floor with or without peri-orbital tissue is resected along with part of the jaw. above others. This may also include skull base resection.
Class IV: Maxillectomy Radical: Maxillectomy with exenteration orbital with or without anterior skull base resection.

Picture 2.8 Illustration maxillectomy with system Liverpool.
Horizontal Components
Type a: resection involving alveoli maxilla unilateral And
palate hard, However No about side contra-lateral And nasal septum .
Type b: maxilla Contralateral resected part with Maxilla ipsilateral.
Type c: jaw on alveolar And palate hard have been completed resected bilaterally.
The transfascial approach allows exposure of the central bony structures. face And can used For tumor in all over area sinonasal. Tumors that have limited extension to the base of the skull are also possible accessed from the direction inferior by method This. There is two type main approach transfacial, namely, the approach rhinotomy lateral And its variations, as well as approach sublabial. Various types approach transfacial, allow access to location sine maxillary, ethmoid sinus, sphenoid sinus, and the three regions of the base structure cranii. However, the indications for the application of this technique have decreased drastically after the advent of the endoscopic approach. 23
On rhinotomy lateral, incision skin started on level cantus medial and continues into the nasofacial and alar-facial sulci to form the wings of the nose. The soft tissues can be retracted to expose the anterior aspect of the maxillary sinus, the piriform openings, and the orbital rim. The infraorbital nerve can be preserved or sacrificed, depending on the carcinologic need. Extension of the skin incision can be performed to expose the anterior aspect of the maxilla more laterally, to the maxillary tuberosity and zygoma. The Lynch incision uses a subbrow split, while the Weber Fergusson incision combines a subciliary split with a labial split. 18,23
Lateral rhinotomy approach providing access to the maxilla, ethmoid, sphenoid, And, when connected with incision Lynch, to sine frontal And anterior aspect of the base of the skull. Lateral rhinotomy may then be combined with a skin incision in the along the lower floor of the orbit and osteotomy of the palate, arch zygomatic, and the maxillary bone below the orbit. Thus, movement jaw on can done For give access wide to the base of the skull, infra-temporal fossa, and carotid artery. 18.23
On approach sublabial, incision made as high as mucosa vestibule on, straight down to the bone, and exposure is done with elevate the periosteum and soft tissues in the same manner as in lateral rhinotomy approach. Therefore, the primary importance of The sublabial approach is to allow access to the subskeletal framework. center of the face while avoiding skin incisions, but exposure is often greater limited compared to the transfascial approach. The sublabial approach which is done in context oncologist on basically is approach Red The Denker And degloving.

Picture 2.6 Illustration area incision on Handling Tumor Sinonasal with access external surgery, transfascial approach.
Note : 1. Lateral Rhinotomy (line intermittent black)
Incision Weber Ferguson (Lateral Rhinotomy + Subciliary Split (blue dotted line) + Labial Split (blue dotted line) yellow dotted ))
Incision Lynch (line intermittent green)
Incision Coronal (red dotted line )
Approach degloving started with incision sublabial bilateral from one tuberosity maxilla to tuberosity maxilla other. Periosteum and network The soft tissue is elevated to the orbital rim, preserving the infraorbital nerve. The incision circular made in room front hole nose And network soft can reclined to superior so that show aspect front jaw on
And framework nose. Depends on location tumor, antrostomy can be done on jaw on, or in a number of case, osteotomy Lefort I for exposing tumors. 18,23,32
Modification lynch ( Neel Lake ) is technique surgery Which started from the nose. The nasal membrane obstruction will be opened and continued with the examination. At procedure this will be done ethmoidectomy intranasal before external surgery is performed. Sometimes this helps adequate communication with the frontal sinus and helps eliminate the tumor. This technique is divided into two stages, in the first stage sphenoid sinus curettage is performed and sine maxillary. After done curettage, so incision will done until it reaches the eyebrow. The lacrimal bone will be removed to allow access to the floor of the frontal sinus. The important difference between Modified Lynch and Lynch is that in this technique, the frontal process of the superior maxillary is maintained to prevent collapse of the orbital part medially, maintaining some of the floor of the frontal sinus (if possible) as well as to prevent protrusion of the contents of the orbital cavity upwards because protrusion can cause the formation of a non-draining pocket in the lateral part of the frontal sinus. 32
A number of writer report use chemotherapy And radiation benefit in further malignancies. Several studies have investigated the role of chemotherapy neoadjuvan in handling karsnona sinonasal stadium continued. Intra-arterial cisplatin combined with intravenous paclitaxel and ifosfamide in patients with locally advanced sinonasal carcinoma has been under review in Center Studies Cancer Anderson For determine efficacy, level and safety. Although these studies showed better organ survival, major toxicities were also reported. 1,15
Radiation is used as a method to assist surgery. Patients with prognosis Which bad Which No Can done action operation should using a combination protocol of chemotherapy and radiation. 9,20 Chemo-radiation therapy is simultaneously can used for patients with condition medical that surgery is not possible if the patient is in good initial condition to undergo multimodal therapy. All decisions on choosing a treatment regimen still depend on the patient's initial condition before starting therapy, such as the quality of kidney function.
Prognosis
Prognosis malignancy This on generally not enough Good Because part Most patients come at an advanced stage. According to Popovic et al., as quoted by Firdaus et al., reported 5-year survival rates for nasal, maxillary sinus, and ethmoid malignancies were 45%, 38%, and 13%, respectively. 10,11
CONCLUSION
Sinonasal carcinoma is the second most common head and neck malignancy after nasopharyngeal carcinoma. Squamous cell carcinoma (SCC) is the most common type of head and neck carcinoma. SCC is divided into two, namely keratin SCC (KSCC) and non-keratin SCC (NKSCC) and most sinonasal SCC are KSCC. The initial symptoms that appear are not specific and symptoms in advanced stages depend on the location and extent of the lesion. SCC is most commonly found on sine maxillary. CT scan is inspection support Which good and is considered the gold standard for the diagnosis of sinonasal SCC. Surgery is the primary treatment for this condition and can followed by adjuvant chemo-radiotherapy in advanced stages. Maxillectomy is an operation performed on advanced stage tumors. carry on. Election technique operation need consider description pre-operative tumor Approach Weber Ferguson And incision Lynch can used to expand access to the skull base as in this case where the tumor has already spread (stage IVB)
REFERENCE
Liorente JL, Lopez F, Suarez C, Hermsen MA. Sinonasal Carcinoma: Clinical, Pathological, Genetic and Therapeutic Advances. Nature Reviews Clinical Oncology. 2014;11:460-72.
Lango MN. Surgery in the Multimodality Treatment of Sinonasal Malignancies. Curr Probl Cancer. 2010; 34(5):304-21.
Gibson TN, McNaughton DP, Hanchard B. Sinonasal Malignancies: Incidence and Histological Distribution in Jamaica, 1973-2007. Cancer Causes Control. 2017; 28:1219-25.
Carrau R. Malignant Tumors of the Nasal Cavity Treatment and Management. Otolaryngology and Facial Plastic Surgery. 2019;1-18.
Probst R, Grevers G, Iro H. Anatomy, Physiology and Immunology of the Nose, Paranasal Sinuses and Face. In: Probst R, Grevers G, Iron H, eds. Basic Otorhinolaryngology. New York: Georg Thieme Verlag; 2006; 2-14.
Warmald JP. Vascular Anatomy of The Nose. In: Byron J Bailey. Head and Neck Surgery-Otolaryngology. 4th ed. Lippincott Williams & Wilkins. 2006; 506- 8.
Leung RM, Walsh WE, Kern RC. Sinonasal anatomy and physiology. In: Johnson JT, Rosen CA, eds. Head & Neck Surgery-Otolaryngology. 5th ed. Philadelphia: Lippincott Williams & Wilkins. 2014; 359-70.
Firdaus MA, Rahman S. Paranasal sinus tumor with intracranial extension and lung metastasis. Department of ENT-KL, Faculty of Medicine, Andalas University. 2012; 1-8.
Haerle SK, Gullane PJ, Witterick IJ, Zweifel C, Gentili F. Sinonasal carcinoma epidemiology, pathology and management. Neurosurg Clin N Am. 2013; 39- 49.
Zimmer LA, Carrau RL. Neoplasms of the nose and paranasal sinuses. In: Johnson JT, Rosen CA, eds. Head & Neck Surgery-Otolaryngology. 5th ed. Philadelphia: Lippincott Williams&Wilkins, 2014; 2044-6
Robinson, AD, Liang, J, Lou, Q. Tumors of the Nose and Paranasal Sinuses. In Diseases of the Sinuses. Springer. New York. 2014:535- 555.
Trivedi N. Tumors of the Nose and Paranasal Sinuses. In Atlas of Head and Neck Cancer Surgery. Springer. India. 2015:171-198.
Thapa, N, Pradhan B. Sinonasal Inverted Papilloma. Journal of the Institute of Medicine. 2013;34(2):10-13.
Reddy NV, Kumari KA, Rathod JBS, Kaur PA, Reddy DS. Rare (R), Malignancies (M), Nose (N), Paranasal Sinuses (PNS), Management (M), Diagnostic Nasal Endoscopy (DNE). Study of Diagnosis and Management of Malignant Neoplasms of the Nose and Paranasal Sinuses: Our Experience. 2016.
Miller ED, Blakaj DM, Swanson BJ, Xiao W, Gillison ML, Wei L, Bhatt AD, Diavolitsis VM, Wobb JL, Kang SY, Carrau RL. Sinonasal adenoid cystic carcinoma: Treatment outcomes and association with human papillomavirus. Head & neck. 2017 Jul;39(7):1405-11.
Ghani NM, Shukri NM, Mohamad A. 2 Case reports of sinonasal adenoid cystic carcinoma: Reviews of the literature on surgical approaches. Egyptian Journal of Ear, Nose, Throat and Allied Sciences. 2016 Nov 1;17(3):173-6.
Trope M, Triantafillou V, Kohanski MA, Kuan EC, Tong CC, Patel NN, Maina IW, Carey RM, Workman AD, Palmer JN, Adappa ND. Adenoid cystic carcinoma of the sinonasal tract: a review of the national cancer database. InInternational Forum of Allergy & Rhinology 2019 Apr (Vol. 9, No. 4, pp. 427-434).
Amen MB, Edge SB, Green FL. AJCC Cancer Staging Manual. 8th Edition. American College of Surgeons. Springer. New York. 2017:53-65.
Aparna C, Renuka IV. Sinonasal Undifferentiated Carcinoma-A Case Report. International Journal of Otolaryngology and Head & Neck Surgery. 2014; 3: 382-6.
Lee JT, Chiu AG. Endoscopic The Denker approach for front maxilla tumors. In Atlas of endoscopic sine and skull base surgery 2019 Jan 1 (pp. 183-190). Elsevier.
Denker A. Ein neuer wegfur die operation der malignen nasentu moren. Munch Med Wochenschr. 1906;20:953–956.
Sturmann D. Die Intranasale Eroffnung der Kieferhohle. Berl klin Wochen schr. 1908;45:1272–1274
Chatelet F, Simon F, Bedarida V, Clerc N Le, Adle-Biassette H, Manivet P,et a. Surgical management of sinonasal cancer: A comprehensive review. Vol. 13, Cancer. MDPI AG; 2021.
Lee JT, Suh JD, Carra R, et a. Endoscopic Denker's approach for resection of lesions involving the anteroinferior maxillary sinus and infratemporal fossa. Laryngoscope. 2017;127:556–560.
Ashman A, Psaltis AJ, Wormald PJ, Tan NC. Extended endoscopic approaches to the maxillary sinus. The Journal of Laryngology & Otology. 2020 Jun;134(6):473-80.
Slow Twig PJ, Ferlito A, Village A, Thompson LDR, Hunt JL, Strojan P, et al. Sinonasal tumors: a clinicopathologic update of selected tumors. Eur Arch Otorhinolaryngol. 2013 Jan;270(1):5–20.
Lewis JS. Sinonasal Squamous Cell Carcinoma: A Review with Emphasis on Emerging Histologic Subtypes and the Role of Human Papillomavirus. Head Neck Pathol. 2016 Mar;10(1):60–7.
Bracigliano A, Tatangelo F, Perri F, Di Lorenzo G, Tafuto R, Ottaiano A, et al. Malignant Sinonasal Tumors: Update on Histological and Clinical Management. Curr Oncol. 2021 Jul 1;28(4):2420–38.
Mahmoud AM, Said A, El Dessouky I, Swede AH, Amen A. Tips and tricks in surgical management of maxillary sine tumors. Egypt J Ear Nose Throat Allied Sci. 2017 Mar;18(1):43–8.
Thawani R, Kim MS, Arastu A, Feng Z, West MT, Taflin NF, et al. The contemporary management of cancers of the sinonasal tract in adults. CA Cancer J Clin. 2023 Jan;73(1):72–112.
Ferrari M, Taboni S, Carobbio ALC, Emanuelli E, Maroldi R, Bossi P, et al. Sinonasal Squamous Cell Carcinoma, a Narrative Reappraisal of the Current Evidence. Cancers. 2021 Jun 7;13(11):2835.
Chatelet F, Simon F, Bedarida V, Le Clerk N, Adle-Biassette H, Manifest P, et al. Surgical Management of Sinonasal Cancers: A Comprehensive Review. Cancers. 2021 Aug 8;13(16):3995.
Neel HB, McDonald TJ, Facer GW. Modified lynch procedure for chronic frontal sinus diseases: Rationale, technique, and long term results. The Laryngoscope. 1987 Nov;97(11):1274–9.
Elgart K, Faden DL. Sinonasal Squamous Cell Carcinoma: Etiology, Pathogenesis, and the Role of Human Papilloma Virus. Vol. 8, Current Otorhinolaryngology Reports. Springer Science and Business Media BV; 2020. p. 111–9.
Siew SS, Martinsen JI, Kjaerheim K, Sparén P, Tryggvadottir L, Weiderpass E, et al. Occupational exposure to wood dust and risk of nasal and nasopharyngeal Cancer: A case control study among man in four Nordic countries—With an emphasis on nasal adenocarcinoma. Int J Cancer. 2017 Dec 15;141(12):2430–6.
Comments