Gentamicin Ototoxicity
I Made Nudi Arthana
Gentamicin ototoxicity can be defined as gentamicin which has the potential to cause toxic reactions in structures in the inner ear such as the cochlea. And vestibule. Damage on structures This Which due to by using the drug can cause symptoms such as hearing loss, tinnitus and disturbance balance. Ototoxicity defined as damage in the cochlear and/or vestibular structures in the ear due to exposure to chemicals 1.
LITERTURE REVIEW
Anatomy And Ear Physiology
Anatomy Ear
The ear is an organ located on the lateral part of each side of the head and plays a role in hearing and body balance. The anatomy of the ear is generally divided into three parts, namely the outer ear, middle ear, and inner ear (Figure 1). 3,4
Ear outside
The outer ear consists of the pinna (ear flap) and the external acoustic canal. Pinna arranged on cartilage And fully coated by network skin. The pinna functions to capture and collect sound waves from the external environment. The external acoustic canal is a 4 cm long channel that play a role in wave transmission sound from environment outside to tympanic membrane. Channel acoustician external divided become two part. One third The outer part of the external acoustic canal is made of cartilage and has hair, sebaceous glands, and sweat glands, all of which play a role in producing earwax. This earwax acts as a protective barrier for the ear. The inner two-thirds of the external acoustic canal is made of bone covered by by network epithelium. Ear outside And ear middle restricted by tympanic membrane. 3.4
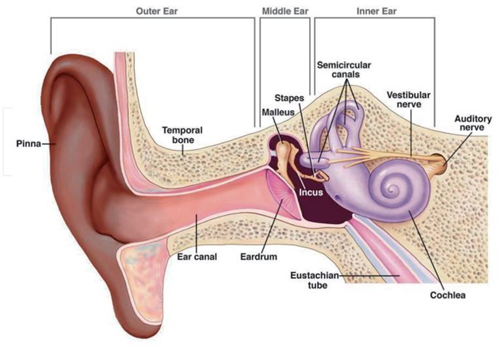
Picture 1. Structure Human Ear Anatomy . 4
Ear Middle
The middle ear consists of the tympanic membrane, the auditory ossicles , the tensor tympani muscle, and the stapedius muscle. The tympanic membrane is cone-shaped and is called the umbo. Based on its morphology, the tympanic membrane is divided into two parts, namely the pars tensa and the pars flaccida (Figure 2). The pars flaccida is located in part superior from membrane timpani in on malleolar fold And arranged on two layers, namely the squamous epithelial and mucosal layers, while the pars tensa consists of three layers, namely the squamous epithelial, mucosal and fibrous layers. The overall structure of membrane timpani This own thickness around 0.1 mm with diameter around 1 cm. Next, there is a tympanic cavity in the middle ear. This tympanic cavity is limited by promontory on side medial, membrane timpani on side lateral, the eustachian tube orifice anteriorly, the aditus ad mastoid antrum posteriorly, the tegmen timpani fossa skull on part superior, And bulb vein jugular on inferior part. Cavity timpani This containing air And relate with cavity nasal through the eustachian tube. In addition, there are three auditory bones ( ossicles ) in the tympanic cavity, namely the malleus, incus, and stapes, which are interconnected with each other. Processus long malleus attached on part in tympanic membrane, whereas stapes attached at the foramen ovale ( oval window ) Which is channel Which related to the vestibular system of the cochlea in the inner ear. 3.4
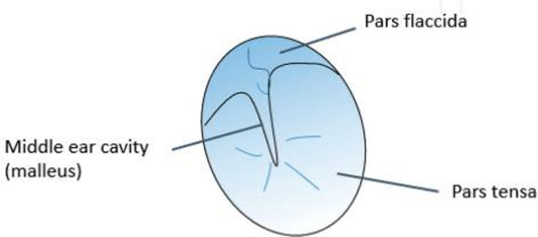
Figure 2. Membrane Structure Timpani. 4
Inner Ear
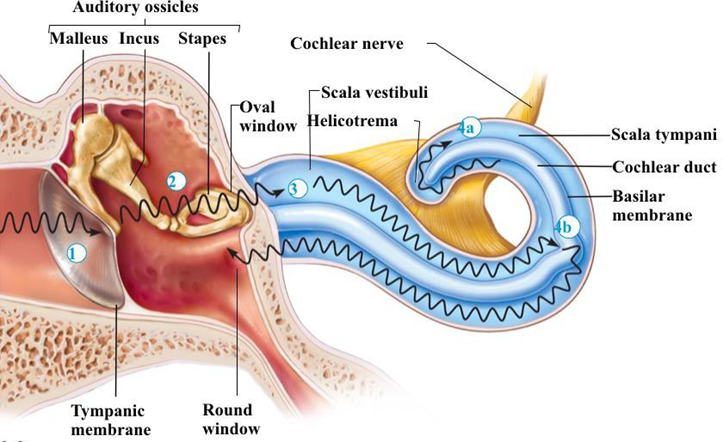
Ear in is at between ear middle And canal acoustician internal and in the petrous portion of the temporal bone. These inner ear structures are referred to as the labyrinth Which divided become three part. Labyrinth bone consists of over the semicircular canals, vestibule, and cochlea. The membranous labyrinth consists of the semicircular ducts, sacculus, utricle, And duct cochlear. Room between labyrinth The bony and membranous labyrinths are filled with perilymph fluid obtained from the lymphatic system (similar to aqueous humor and cerebrospinal fluid). The interior of the membranous labyrinth is also filled with a fluid called endolymph produced by dark cells located in the cochlea. Perilymph and endolymph fluids have different compositions. Perilymph fluid is rich in sodium but low in potassium, whereas endolymph fluid has a high potassium content. The utricle and saccule act as otolith organs that have a neuroepithelial layer so that they can interact with endolymph fluid to trigger the depolarization of the stimulus needed in vestibular function. The cochlea is a canal structure formed from bone and lined by epithelial tissue. The cochlea has form resemble snails and play a role important in function hearing. Cochlea consists of from three channel (scala vestibuli, scala tympani, and scala media). Scale vestibuli and scale fluid filled tympanic membrane perilymph, whereas scale media containing fluid endolymph. There is a the membrane that separate vestibular scale and media scale which are called Reissner's membrane, while the membrane that separate scale timpani And The media scale is called the basilar membrane. The cochlea also has an organ of Corti in it. The organ of Corti is a sensory organ located on the basilar membrane and functions to convert sound energy into nerve stimuli so that it plays an important role in hearing function (Figure 3). The organ of Corti has hair cells (mechanosensory cells) and a tectorial membrane. In total, there are about 3,000 inner hair cells and 12,000 outer hair cells in the organ of Corti. These hair cells are stereocilia Which own arrangement, size, And stiffness Which different and respond to sound stimuli with different frequencies. These hair cells are embedded in the tectorial membrane. These hair cells convert sound energy into nerve stimuli that are conducted to the cochlear nerve. 3.4
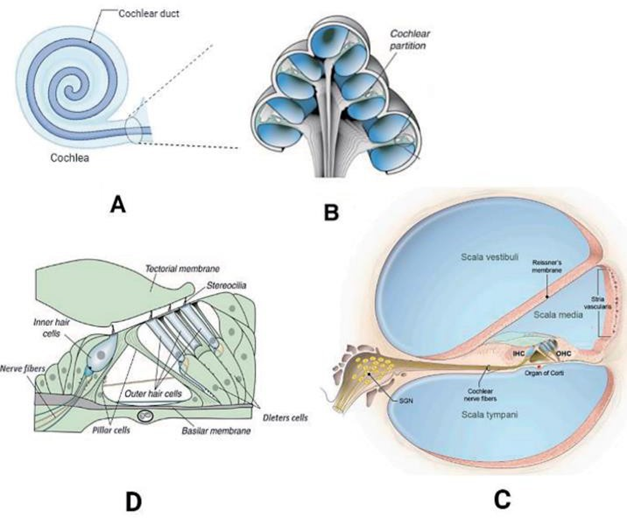
Picture 3. Structure Cochlea. 4
The vascularization of the external ear (pinna and external acoustic canal) is carried out by the posterior auricular artery, the superficial temporal artery, and the deep auricular artery (specifically canal acoustician external just), whereas drainage done by combination superficial temporal vein, posterior auricular vein, and mastoid emissary veins (MEV's). The pinna is innervated by branches of cranial nerves V, VII, IX and X, while the canal acoustician external get innervation from branch nerve cranial VI And
X. The tympanic membrane receives vascularization from the posterior auricular artery and branches of the deep auricular artery, while its drainage is to the maxillary and jugular veins. external And plexus venous pterygoid. Membrane timpani innervated by by branch from nerve cranial X, XII, And VI. Supply blood For cavity timpani done by artery timpani anterior, artery stylomastoid, artery Petrol superficial, artery inferior tympanic membrane, whereas the drainage done by vein Which culminate on sine superior petrosal and plexus pterygoid. The inner ear (cochlea) receives its vascular supply from the internal auditory artery which is a branch of the anterior inferior cerebellar artery (AICA). This vascular supply in the cochlea will then form a microvascular network on the lateral wall of the cochlea. There are two microvascular networks, namely the microvascular network in the striae vascularis and the microvascular network in the spiral ligament (Figure 4). 5,6
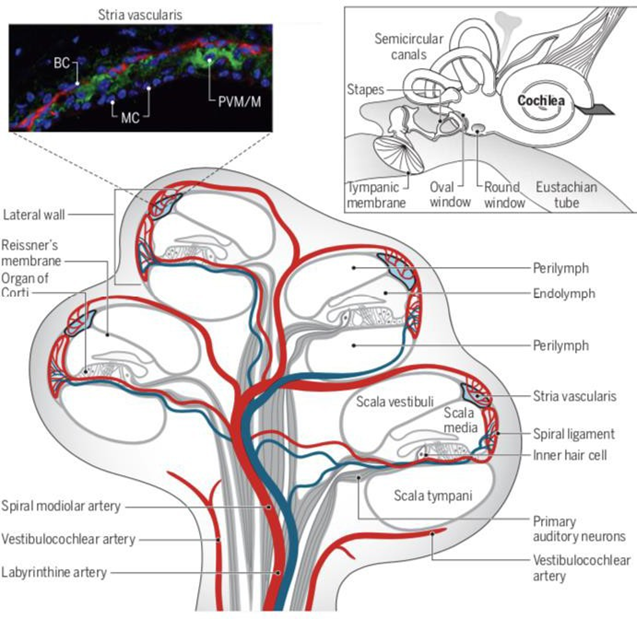
Picture 4. Vascularization Cochlea. 5
Physiology Hearing
The ear is an important organ in hearing and balance (vestibular) function. Hearing is process physiology Which change wave voice from the external environment into nerve impulses which can then be interpreted by the cortex. brain. Wave voice will collected and was captured by pinna and is channeled to the tympanic membrane after passing through the external acoustic canal. The human ear can detect And catch wave voice with frequency 20-20,000 Hz And intensity from 0-130 dB 4.5 . Sound waves that reach the tympanic membrane will then be converted into vibrations. These vibration waves will be transmitted from the tympanic membrane to the inner ear through the auditory ossicles. The vibration stimulus from the auditory ossicles will then vibrate the foramen ovale so that mechanical vibration waves This will changed become wave vibration fluid perilymph on cochlea.
Furthermore, vibration This will delivered to endolymph through membrane Reissner. The movement or vibration of the endolymph will stimulate the basilar membrane of the cochlea, causing depolarization of the hair cells in the organ of Corti. Depolarization of stereocilia cells (hair cell) on organ corti This will cause release neurotransmitters so that The nerve impulses are then transmitted to the cochlear nerve. These nerve impulses will to be continued to the VIII cranial nerve until it reaches the auditory cortex temporal lobe where sound will be interpreted (Figure 5). 4,5
Aminoglycosides
Since being introduced in 1944, several aminoglycoside preparations have been available in Indonesia, including streptomycin, kanamycin, gentamicin, neomycin, tobramycin, netilmicin, And amikacin. Aminoglycosides is antibiotics bactericidal binding ribosome 30S and inhibits bacterial protein synthesis, but only against bacteria basil aerobic grams negative And staphylococcus. Isolation beginning streptomycin from Streptomyces griseus provides long-term therapy for tuberculosis and is an effective antibiotic against gram-negative bacteria. In subsequent years , other aminoglycosides have been isolated from Streptomyces spp ., generally associated with the suffix “mycin” in their nomenclature. Aminoglycosides are also often combined with penicillin on case endocarditis staphylococcus, streptococcus, and especially enterococcus. The combination of aminoglycosides with beta-lactam antibiotics is used in serious pseudomonas aeruginosa infections 7 .
Aminoglycosides including Wrong One class antimicrobial Which conventional. Therapeutic window Which narrow And nature nephrotoxic, ototoxic as well as presence antibiotic Broad-spectrum antibiotics such as cephalosporins, carbapenems, and fluoroquinolones have limited the use of aminoglycosides in the last two decades. Their superiority against multidrug-resistant gram-negative pathogens such as pseudomonas aeruginosa and Acinetobacter spp , price Which cheap, as well as resistance Which low is reason This drug is still used 8,9 .
Aminoglycosides are excreted through the kidneys as intact compounds, via glomerular filtration. Aminoglycoside clearance is similar to creatinine clearance and is reduced in conditions function kidney Which bad. By Because That, clearance aminoglycoside Also reduce in the elderly and neonates. Its concentration in the urine of the elderly and neonates is 70% of the dose given or even more, therefore this drug is ideal for administration on treatment infection channel urine. Time beak its elimination around 2-3 hours in adults and prolonged in children, especially neonates due to their immature renal function, as well as in end-stage renal disease 23 .
Aminoglycosides are hydrophobic polycationic molecules, their cationic nature results from the dominance of ionizable basic amino groups in their chemical structure. They have bactericidal activity through the disruption of bacterial protein synthesis. Due to their cationic nature, aminoglycosides are not lipophilic (fat-soluble) and therefore have very poor absorption from the gastrointestinal tract, resulting in oral administration of aminoglycosides No recommended. By Because That, drug This need given in a way intramuscular or which are more general through route intravenously. After giving parenteral, volume distribution aminoglycosides approach the total body volume, with good distribution throughout the tissues, especially to in fluid extracellular Because characteristic its hydrophilicity. Volume The distribution (Vd) of gentamicin decreases with age. The volume of distribution of gentamicin varies from 0.5–0.7 L/kg on baby premature until 0.25 L/kg on mature young, because of the proportions total water body Which more tall on neonate. They own penetration Which good to a number of fluid body including fluid synovial, peritoneal, ascites, And fluid pleura, but its penetration is poor into the central nervous system and vitreous. Aminoglycosides are distributed quite slowly into bile, feces, prostate, and amniotic fluid. The volume of distribution increases in conditions such as sepsis, severe burns, febrile neutropenia, congestive heart failure, peritonitis, post partum and on parenteral administration 10,11,12 .
Aminoglycosides enter cells through electrostatic binding of their positive molecules to the components negative surface cell bacteria (lipopolysaccharide) And phospholipids on membrane outer membrane of gram-negative bacteria and phospholipids and teichoic acids in gram-positive bacteria). This binding allows access to the periplasmic space. Anaerobic bacteria are generally resistant to aminoglycosides due to the lack of membrane potential and electron transport mechanisms necessary for drug uptake. From the periplasmic space, small amounts of aminoglycosides cross the inner membrane and enter the cytoplasm. In the cytoplasm, they affect protein synthesis by inhibiting translation initiation, blocking elongation translation or cause error codon reading. Process This leading to formation protein Which Wrong translated so that cause damage on the inner membrane of the bacteria. This event facilitates the uptake of other aminoglycosides, which accumulate in the cell and accelerate the process of mistranslation, resulting in murder bacteria dependent on concentration by aminoglycoside
10,11,12 .
Aminoglycoside toxicity includes nephrotoxicity and ototoxicity. Nephrotoxicity occurs in 5%-25% of patients receiving aminoglycosides in divided doses. The incidence of aminoglycoside ototoxicity is still controversial, in some studies mentioning the figure of 3%-41% for hearing loss, while vestibular disorders occur in 1%-11% 1,3,4 . Aminoglycosides are compounds consisting of two or more sugars amino Which bound in a way glycosidic on core hexose. Hexose the called aminocyclitols, namely streptidine (in streptomycin) or 2-deoxycystreptamine (characteristic of bonds in other amino-glycosides), are polycationic compounds which are strongly basic and very polar, both in basic form and in salt form 2,10 .
The antibacterial activity of gentamicin, tobramycin, kanamycin, netilmicin, and amikacin is mainly against aerobic gram-negative bacteria, while the activity against microorganisms or facultative bacteria in anaerobic conditions is very low. Streptomycin and gentamicin are active against enterococci and streptococci other than S. pneumoniae and S. pyogenes . on level Which in a way clinical only can achieved when merged with Penicillin. Aminoglycosides work by inhibiting bacterial protein synthesis. Most antibiotics that work by inhibiting bacterial protein synthesis are bacteriostatic but aminoglycosides are bactericidal. Bacteriostatic antibiotics only inhibit the growth of bacteria And No turn off, whereas bactericidal can kill bacteria. The speed of antimicrobial activity depends on the concentration of the drug, the higher the concentration of the drug so the more fast ability For kill bacteria. Working mechanism aminoglycoside is at first with diffuse free through channel water outer membrane of gram-negative bacteria, then enter the cytoplasmic space. Transport into the membrane in cytoplasm This need energy, Which divided become two phase that is phase I and II. Phase I can be blocked by Ca 2+ and Mg 2+ , hyperosmolarity, decreased pH, and anaerobiasis. This can explain why in an acidic or anaerobic environment (for example in an abscess), aminoglycoside activity decreases. Once inside the cell, aminoglycosides will bind to polysomes (for streptomycin, especially in the 30S subunit) and interfere with protein synthesis by causing "RNA misreading" so that premature termination occurs in the mRNA translation process. This imperfect protein is inserted into the cell membrane, causing increased membrane permeability and stimulating further aminoglycoside transport. This aminoglycoside transport phase is called phase II, the mechanism of which is related to damage to the cytoplasmic membrane structure so that there is leakage of ions which ultimately also causes protein leakage, causing death induced by the aminoglycoside. Aminoglycosides other than streptomycin, for example neomycin, kanamycin and gentamicin can interact on more from One subunit ribosome (No only subunit 30S but Also subunit other for example 50S), so that function ribosome Which disturbed more wide And its antimicrobial potential exceeds that of streptomycin 2,10,11,12 .
Epidemiology
On a number of country, antibiotics can prescribed in a way free even available without a prescription. In this area, aminoglycosides can cause 66% of cases of deafness. Found 33% of cases of adult patients with audiometric changes on administration aminoglycoside depends dose And long therapy. Toxicity vestibular reported on 4% case. Incident patient Which experience toxicity Because aminoglycoside reported to decrease with increasing awareness and monitoring during therapy 2,14 .
Factor Risk
There are several risk factors that increase the risk of ototoxicity associated with dose tall, level drug in blood, And term time therapy. Factor risk others are related to patient age, renal function, hearing loss, family history of ototoxicity, loop diuretics, or other ototoxic drugs. Genetic predisposition is the presence of a mutation in the RNA gene 1555A>G which is often found in association with aminoglycoside-related hearing loss. This mutation causes changes in mitochondrial protein synthesis. In Asian patients with this mutation, aminoglycoside ototoxic symptoms appear more quickly. A detailed evaluation of family history is very important and can be useful in preventive efforts. cases of this gene mutation are also often found in patients with cystic fibrosis and other dysfunctional systems 14,15 .
Toxodynamics Aminoglycosides
Aminoglycoside antibiotics generally have the same mechanism of action and spectrum of action. germs, absorption, elimination, potential ototoxic and nephrotoxic Which The same. Therefore That all antibiotic group This show pattern effect side Which The same although the frequency and degree of side effects caused by each aminoglycoside vary (Table 1) 16 .
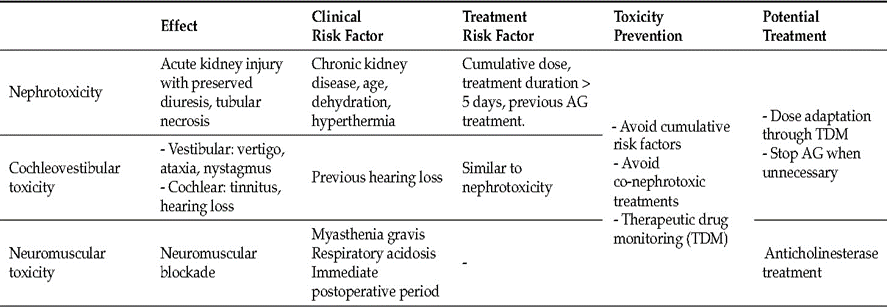
Table 1 . Effect side aminoglycoside
In general general, aminoglycoside used as therapy febrile neutropenia, infection heavy in ICU, sepsis or septic shock, tuberculosis, surgical prophylaxis, prevention of secondary infections on condition chronic like cystic fibrosis, endocarditis bacterial, osteomyelitis and complications of abdominal infections caused by gram-negative bacteria 8,17 . Head and neck infections for which this class of drugs is used include acute and chronic sinusitis, acute otitis media, deep neck abscesses and infected cholesteatoma 18
Streptomycin and kanamycin are highly toxic to both the cochlea and the vestibule, but these two antibiotics are still used for the treatment of tuberculosis and the ototoxicity that occurs. on around 20% sufferer tuberculosis Which accept therapy with drug 17. Gentamicin, tobramycin, and amikacin are anti-pseudomonal aminoglycosides. Gentamicin often used as antibiotics prophylaxis before surgery. Matter This does not pose an ototoxic risk. Neomycin is the most cochleotoxic aminoglycoside of all drugs in its class, therefore it is for topical use only 18 .
Aminoglycosides have excellent ability against Eschericia coli, Klebsiella pneumonia and Enterobacter spp and the resistance rate of aminoglycosides against these pathogens is very low in various parts of the world. Aminoglycosides (especially amikacin) together with carbapenem And polymyxin own activity Which very good against multidrug-resistant organisms such as Pseudomonas aeruginosa and Acinetobacter spp 17,18 . The following is a description of the types of aminoglycoside drugs that are effective against types of germs and diseases and their preparations available in Indonesia. (Table 2)
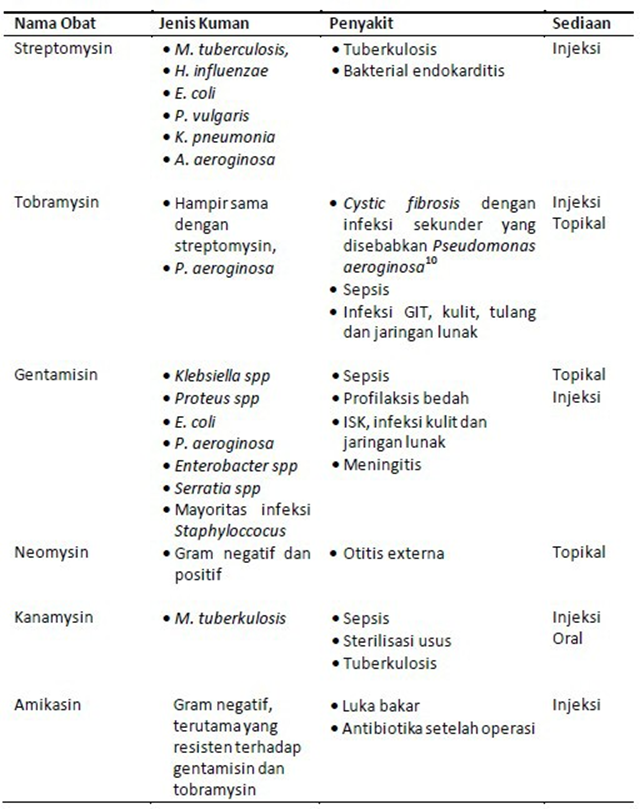
Table 2 . Drug Name, Sensitivity To Germs, Disease And Preparation
Pharmacokinetics Aminoglycosides
Aminoglycosides enter the inner ear rapidly after administration by intravenous injection. The drug can be found in the inner ear within minutes after injection And reach effect plateau 30 minute until 3 O'clock after giving. T½ aminoglycoside in vessels blood achieved around 3–5 O'clock Then, but in fluid inner ear remains found months after therapy is stopped 22 . Aminoglycosides are not easily absorbed in oral administration because they are not soluble in fat so that absorption in the intestine is very slow and difficult to penetrate the lipid layer in the cell membrane, but are very soluble in water. Alkaline conditions increase antibacterial activity, conversely acidic environments (eg in the stomach) decrease their activity 9,16 .
Aminoglycosides are excreted through the kidneys so that in the case of decreased kidney function the dose should be reduced or preferably stopped. This class of drugs does not penetrate the blood-brain barrier. Aminoglycosides have an effectiveness that depends on the concentration of the drug, where the drug kills bacteria more quickly and efficiently when given at high concentrations. This can be achieved with 1 dose compared to 2 or 3 doses in one day (dose dependent) 28 .
Interaction of aminoglycosides with loop diuretics can increase the potential for ototoxicity of this class of drugs because it increases the permeability of the striae vascularis so that the concentration of the drug in the media scale increases. A single dose of ethacrynic acid or mannitol given together with kanamycin can result in severe permanent hearing loss 20 . Renal toxicity is generally reversible because renal tubular cells can proliferate and replace cells damaged by aminoglycosides, but ototoxicity is generally permanent because inner ear hair cells do not have the same ability as renal tubular cells. The nephrotoxic and ototoxic properties make antibiotics included in the aminoglycoside class not recommended for pregnant women 11 .
Aminoglycosides themselves are bactericidal that work in several parts of bacterial cells. First, in the cation part of this antibiotic binds to the anion on the outside of the membrane of gram-negative organisms, thereby disrupting the integrity of the bacterial cell wall and disrupting the permeability function of the bacterial cell wall. Second, aminoglycosides inhibit bacterial protein synthesis by binding to the 30S ribosomal subunit, then there is an error in reading the genetic code and inhibition of translocation. The extension of the amino acid chain fails to form so that the bacteria die 9,21 . Ability antibacterial This depends from ability aminoglycoside bother synthesis protein in cell bacteria. Disturbance synthesis protein influence turnover protein And ultimately killing the bacteria 22 .
Systemic administration of aminoglycosides until they enter the cochlea and cause hearing loss begins with the entry of aminoglycosides into the cochlear blood vessels in the striae vascularis and capillary blood vessels in the basolateral wall. In the cochlea there is a blood labyrinth barrier (BLB) or cochlear blood barrier that separates and protects cochlear cells from the entry of macromolecule circulation. And cells blood. BLB This formed from cell endothelium vascular Which connected by tight connection in tightly coupled epithelial cells. The cochlea also contains perilymph fluid, which has a distinctive ionic composition compared to other extracellular fluids (i.e., high Na+, low K+, and millimolar Ca2 + ) and a larger volume of fluid enters the perilymphatic space surrounding the membrane. basolateral cells hair from flow blood, so that aminoglycoside not easy enter to cells hair from domain this is 23 .
In contrast, endolymph has a unique extracellular ionic composition on the apical surface of mammalian hair cells (i.e., high K+, low Na+, and ~20-μM Ca2 + ). Paired epithelial cells surround the smaller endolymph to prevent mixing of endolymph with perilymph and thus prevent hearing loss. The endolymphatic potential and its ionic composition are generated by the metabolically active cells of the vascularized stria vascularis in the lateral wall of the cochlea. Systemically administered aminoglycosides cross the BLB of the stria vascularis more rapidly than the spiral ligament, which is more closely located within the perilymph. In a study by Li & Steyger 2011, aminoglycoside Which given in a way systemic Also enter cells hair more rapidly than when aminoglycosides are infused directly into the perilymph compartment surrounding the basolateral membrane of the hair cells. Systemic inflammation and noise are both associated with vasodilation of blood vessels. in stripe vascular, so that increase absorption aminoglycoside in cochlea 24 .
When aminoglycosides are in the stria vascularis, they penetrate the BLB and enter the endolymph through several mechanisms, including 23,24 :
In the capillary lumen through ion channels / electrogenic sodium symporters mediated by TRP V4 (Transient Receptor Potential Vanilloid type-4) and TRP V1 receptors which increase the absorption of aminoglycosides by hair cells.
Diffusion cell
Transport protein
Transport paracellular (Gap junction)
Absorption of aminoglycosides through the basolateral membrane of marginal cells (Transitosis absorption )
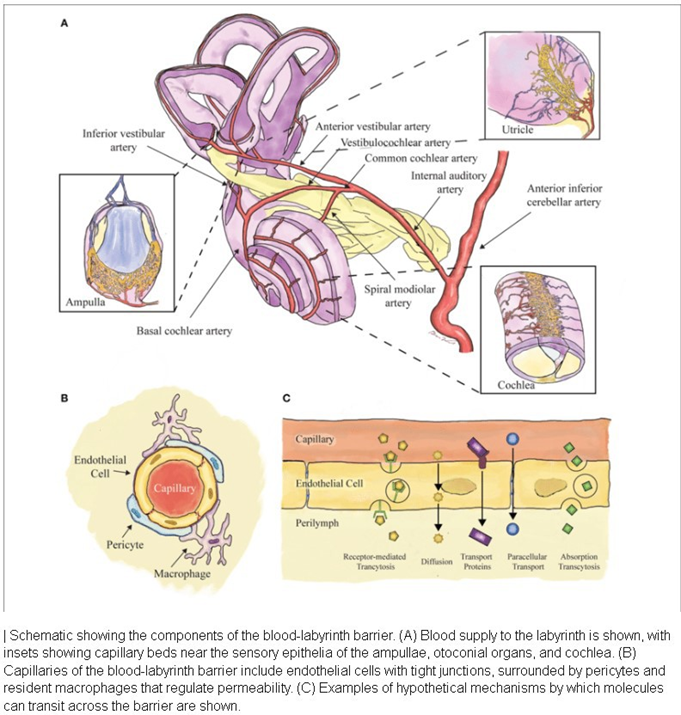
Figure 6. Schematic AMG entering Endlymph via Blood Labyrinth Barrier
After being in the endolymph, aminoglycosides will enter the hair cells in several ways, including: 23,24,25
The MET (Mechanoelectrical Transduction) channel located at the apex of the auditory hair cells, during the depolarization phase of the hair cells, opens the MET channel and causes aminoglycosides to enter the hair cells through the TMC1 (transmembrane channel-like protein-1) channel .
Aminoglycosides enter into the cell hair through channel apical cation cell hair by means of TRPV1 and TRPV4
Aminoglycosides enter through the basolateral membrane of outer hair cells mediated by the TRPA1 (Transient Receptor Potential Ankyrin type-1) receptor.
Aminoglycosides enter through apical endocytosis And cause degradation lysosome
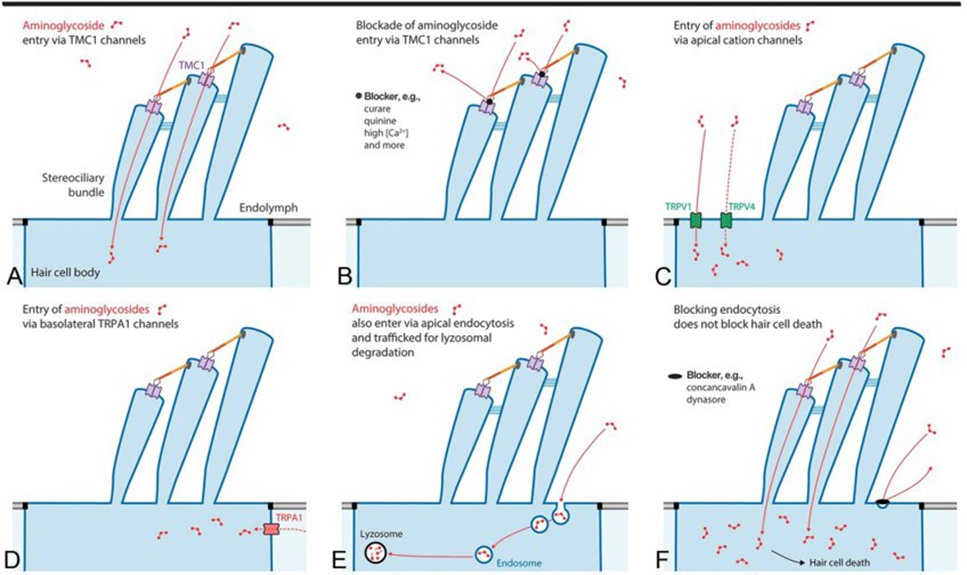
Picture 7. Mechanism AMG's entry into the auditory hair cells
Moment aminoglycoside enter cell hair happen a number of process Which resulting in the occurrence of disturbance hearing. Mechanism in the cells hair hearing that is :
25,26,27
Aminoglycosides bound with PIP2 (Phosphatidylinositol 4,5-bisphosphate) which then blocks the gate voltage of the basolateral membrane of the outer hair cells thereby preventing rapid repolarization of the cells which is crucial for the survival of the auditory hair cells.
Aminoglycosides in the intracellular fluid of the cytoplasm degrade the pre-synaptic ribbon (cholear synaptopathy) in hair cells so that hearing function is lost, even though many hair cells are still alive but have been damaged so that they cannot function normally in the hearing process. 25,26,27
Aminoglycosides damage marginal cells and intermediate cells in the stria vascularis which have a responsible function. answer in maintaining ion concentration Potassium in the endolymph fluid remains high and maintains the positive potential of the endolymph on the media scale high.
Aminoglycosides bind to efferent synapses at the base of the outer hair cells resulting in dysregulation of the olivocochlear reflex, which functions to protect the auditory hair cells from loud sounds.
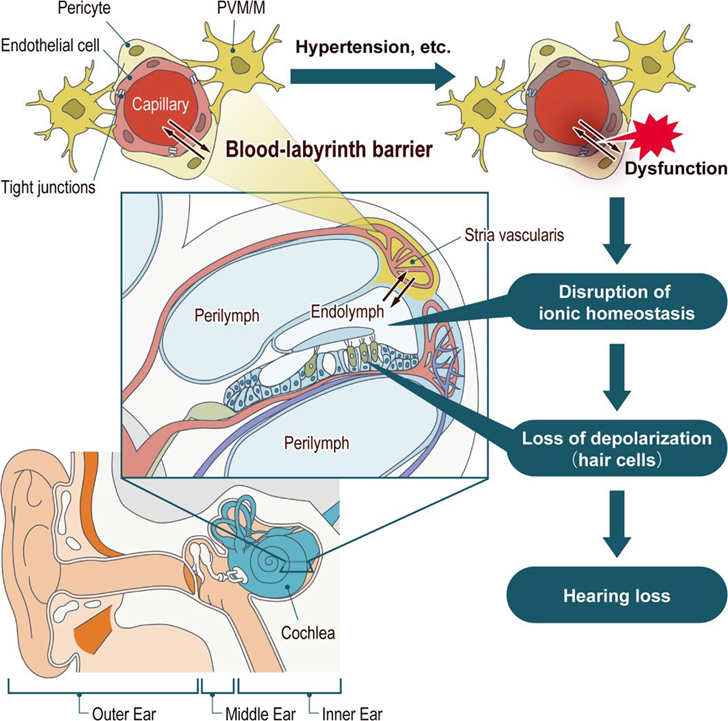
Figure 8. Process disturbance hearing on cochlea
Toxicity Aminoglycosides
Nephrotoxicity
Administration of aminoglycosides for several days can cause mild kidney disorders, which are still reversible. This toxicity is caused by the accumulation and retention of aminoglycosides in the proximal tubule cells 16 . As a consequence, the renin angiotensin system will be activated, causing local vasoconstriction and a decrease in the glomerular filtration rate 22 . Early manifestations of this damage are the excretion of renal tubular brush border enzymes . After several days, there is an abnormality in the ability to concentrate urine, proteinuria light, And formed cylinder hyaline And granular 19 . Potential nephrotoxic aminoglycoside from Which most heavy consecutive is neomycin > gentamicin > tobramycin = amikacin > netilmicin > streptomycin 28 . The glomerular filtration rate also decreases in the following days non-oliguria renal insufficiency is thought to be due to the effect of aminoglycosides on the distal nephron. If acute tubular necrosis occurs, the symptoms that appear are a mild increase in plasma creatinine (0.5-2.0 mg/dl; 40-175 LM). Besides That Also can found improvement level blood urea and decreased creatinine clearance 36 . This renal dysfunction is usually reversible because the proximal renal tubule cells have the ability to regenerate. The occurrence of tubular necrosis due to aminoglycoside administration, namely aminoglycosides, causes toxicity that is directly proportional to the local concentration in the lysosome. Here the lysosome becomes a key location because the lysosome is the place accumulation drug in cell tubule. With thus happen lysosomal changes 31 . These changes are in the form of lysosomal phospholipidosis, which occurs due to the reduction of the negative charge required for the functional activity of phospholipase and inhibition phospholipase A1, A2., And C1 29 . Aminoglycosides become toxic once released the lysosome occurs when the critical threshold of lysosome changes and/or accumulation drug achieved. For example gentamicin will chelate Fe ++ in mitochondria so that the Fe ++ -gentamicin complex is formed which is a free radical. This free radical plays a direct role in causing cell death. In addition, lysosomes release enzymes protease that called cathepsin, in where this enzyme will induce apoptosis which results in cell death 30 . Drugs in lysosomes are basically non-toxic. Toxicity is caused by the influence of aminoglycosides on non-lysosomal targets, such as the apical and basolateral membranes, and changes in these structures will cause cell death. Gentamicin also inhibits enzymes in the cell membrane, namely Na + K + ATPase and releases LDH (lactate dihydrogenase) so that cell death occurs 30. As is known, the Na + K + ATPase enzyme is an important component in the homeostasis of cell components, so that if it is inhibited, cell necrosis or apoptosis will occur. Biochemically, abnormalities that cause damage cells tubular This happen Because change structure mobile membrane.
Aminoglycosides inhibit phospholipase sphingomyelinase and ATPase, and inhibit mitochondrial and ribosome activity. Because of the ability of aminoglycosides to interact with anionic phospholipids, this drug can inhibit the formation of autacoid Which originate from membrane And second messenger intracellular such as prostaglandins, inositol phosphates, and diacylglycerol. These prostaglandin changes can explain the relationship between tubular damage and decreased glomerular filtration rate 16 . Several other experts have stated that aminoglycosides cause change morphological in cells endothelial glomerulus (decreased number of endothelial fenestrae) and decreased glomerular capillary ultrafiltration coefficient 16. In a study on mice given gentamicin and netilmicin for 10 days, it was concluded that mice treated with low-dose gentamicin experienced process apoptosis in some parts of the cortex different, while the use of amikacin did not show such effects. This study also found a cortical proliferative response due to tubular apoptosis induced by aminoglycosides 31 . Another study found that patients without risk nephrotoxicity Which given aminoglycoside during 7-10 day, It turns out that the risk of experiencing nephrotoxicity due to aminoglycosides is equivalent to the risk due to antibiotics. group beta lactam other. For overcome matter This, so It is recommended that aminoglycoside administration be adjusted to the dosage schedule and interval, so as to minimize the risk of toxicity and increase efficacy, especially based on pharmacokinetic and pharmacodynamic considerations 29 .
Ototoxicity
Aminoglycoside ototoxicity is a tendency of aminoglycosides, whether given systemically or topically, to cause decreased function and cellular damage in the inner ear, namely the cochlea, vestibule or vestibulocochlear nerve 20,33,40 . The effects of ototoxicity are generally symmetrical, except in the topical use of aminoglycoside ear drops into the tympanic cavity where ototoxicity Which happen unilateral 41 . A number of factor Which influence ototoxicity is a decrease in function kidney, dosage high, long term use long (more than 10 or 14 days), concomitant administration with ototoxic drugs others such as cisplatin etc., increased serum aminoglycosides, patients over 60 years of age, history of previous sensorineural deafness and history of previous ototoxicity 33,34,35,40,42,43 . This is more clearly seen in the Table below.
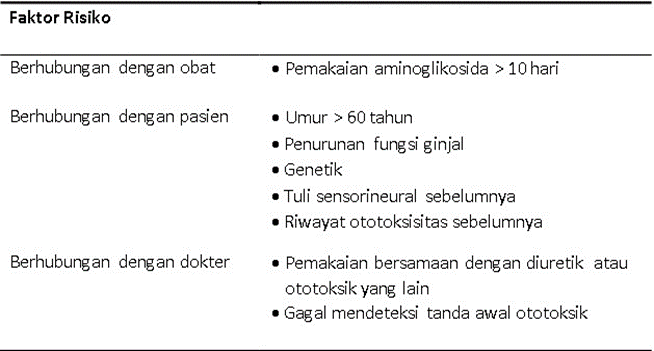
Table 3. Factor Risk Ototoxicity Aminoglycosides
The potential for aminoglycoside ototoxicity is as follows: neomycin > gentamicin = tobramycin > streptomycin = amikacin = kanamycin 35,36 . Ototoxicity is caused by aminoglycosides accumulating in the perilymph and endolymph of the middle ear, and this accumulation occurs mainly when the levels of aminoglycosides in plasma are quite high. Back diffusion of aminoglycosides into the bloodstream is slow, so that their half-life becomes longer (can be up to 6 times that in plasma). The slowness of back diffusion is because drug diffusion depends on concentration. The tendency for damage to cells in the cochlearovestibular varies. Amikacin, tobramycin, and kanamycin tend to damage hair cells in the cochlea (causing hearing loss), while streptomycin and gentamicin are more damaging to vestibular sensory cells (causing balance disorders). This difference in ototoxicity is due to differences in the number of free amino or methylamine groups that bound on part glycoside molecule 32 . Damage cells hair cochleovestibular ototoxicity due to aminoglycosides is usually irreversible. The mechanism of ototoxicity in these cells hair cochlea And vestibular on basically The same. Aminoglycosides interact with phosphatidylinositol in the membrane of hair cells. Aminoglycosides increase membrane permeability, causing Mg 2+ to leave the cell, whereas in normal cells content Mg ++ in mitochondria very tall. Lost Mg2 + causes inhibition in enzymatic reactions (Mg 2+ is needed as a cofactor) resulting in cell death 46 . Phosphatidylinositol and its phosphorylated derivatives are intracellular second messengers as precursors of inositol triphosphate and diacylglycerol. Aminoglycosides can cause loss of cochlear hair cells in the organ of Corti or each of these cells can merge (fusion) into a giant cell. The initial damage occurs at the base of the cochlea (which functions to capture high-frequency sounds) high), and if exposure to aminoglycosides continues, over time damage also occurs to the cochlear apex (for low-frequency sounds). Once the hair cells are damaged, then it can't be done regeneration occurs so that deafness occurs who settled. Process death cell hair This Can happen fast (in time 30-60 minute) or slow, namely 3-6 hours 31 . The existence of this fast and slow process occurs because of the differences in hair cell susceptibility to various types of aminoglycosides, which is caused by the heterogeneity between these hair cells. Symptoms of cochlear ototoxicity begin with hearing loss to high frequency sounds (often not realized by the sufferer), followed by hearing loss to low frequency sounds and finally occurs deafness settled. Symptom early can detected with audiometry. If hearing disorders early the left alone And aminoglycoside still given, so will hearing loss occurs at low frequencies and sufferers begin to have difficulty communicating 32 .
Audiograms in patients with aminoglycoside intoxication show increased thresholds at high frequencies (400 and 8000 Hz or higher), with a progressive increase in threshold frequency Which more low. If drug forwarded so patient will experience permanent deafness, but if stopped immediately partial hearing recovery can occur. Damage is always preceded by tinnitus and it is this tinnitus complaint that is always complained of by patients, not their hearing loss. The mechanism of ototoxicity that occurs in the cochlea, vestibular and auditory nerves can occur due to systemic use And topical 31,32 . Aminoglycosides to form complex with metal transition like iron and copper, this complex is redox active which when reacted with electron donors such as arachidonic acid will form reactive oxygen species (ROS) or free radicals such as superoxide, hydroxyl radicals and hydrogen peroxide. Reactive oxygen species are responsible for cell damage caused by aminoglycosides 37,46 .
Reactive oxygen species cause antioxidant defenses to weaken and alter glutamate balance. Reactive oxygen species will activate c-Jun terminal kinase (JNK). C-Jun-terminal kinase (JNK) affects gene transcription in the nucleus and activates apoptosis and necrosis of Cochlear hair cells. The outer hair cells of the cochlea are more sensitive to free radicals than the inner hair cells and supporting cells. The outer hair cells in the basal part are more sensitive when compared to the apex part 37,47 .
Drops ear Which contain aminoglycoside more often reported causing vestibular toxicity 48 . Ear drops reach the inner ear through several routes, namely through the foramen rotundum membrane, the annular ligament of the stapes, congenital or acquired microfractures, and the last is likely to originate from systemic uptake by the middle ear mucosa 40,49 . Topical ear drops containing neomycin and gentamicin in the case of a perforated tympanic membrane will allow the drug to pass through membrane foramen rotunda, Which is point potential between ear middle and inner ear and finally reaches the membranous labyrinth 33 . Topical skin therapy can cause hearing loss if the treated area is very large because it allows the occurrence absorption systemic Which tall, for example on wound burn Which area and irrigation of peritoneal wounds 35 . Microscopic studies have shown that damage caused by aminoglycosides occurs in the sensory cells of the organ of Corti, the crista ampullaris and macula from sacculus And utricle. Microscope electron show that damage occurs to the first row of hair cells, especially the basal part of the cochlea and ganglion neurons. spiral 33 . Cell hair outside is part Which most prone to caught ototoxicity, but inner hair cells may be affected if aminoglycosides are given in high doses. And giving in term long. Group drug This concentrated in a way selectively in hair cells when located in the perilymphatic space 39 .
The outer hair cells of the organ of Corti are generally the first to show signs of intoxication. Damage varies start from stereocilia Which damaged in surface cell hair until lost all over cell hair, so that Which left behind only A little cell Support. Damage critical marked with the disappearance cell hair part in And cell spiral ganglion. Loss of cochlear hair cells will result in degeneration of the auditory nerve 16. Neomycin, kanamycin, amikacin, sisomycin And dihydrostreptomycin damage cochlea by damage cell hair outside started from part basal And to be continued to direction apex cochlea 34.40 .
The process of vestibular ototoxicity begins with damage to hair cells at the apex of the crista ampullaris. If it continues, the loss of hair cells to the peripheral vestibular receptors, the otoconia membrane and the surface of the otolithic membrane are not spared from damage 49 . Streptomycin, gentamicin and tobramycin selectively damage hair cells in the crista ampullaris, but when given in dose tall Also allow the occurrence damage in the cochlea. Type I hair cells in the vestibule are more vulnerable than type II, the crista ampullaris is more sensitive to toxicity than the macula of the utricle and saccule 16 .
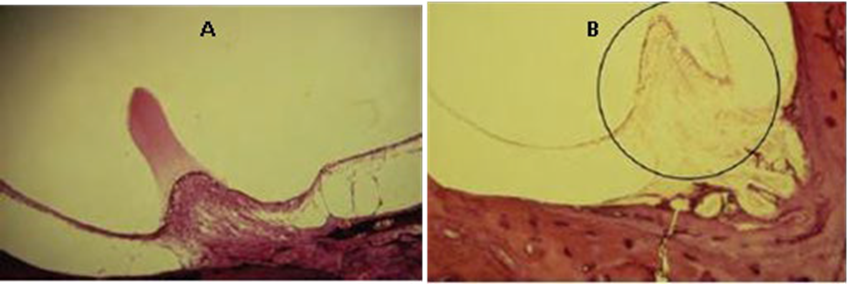
Picture 9 A. Normal Cupula. B. Cupula, cell hair hearing type I And type II disappeared due to gentamicin ototoxicity in the ampulla 40
Diagnosis
In establishing the diagnosis of patients with ototoxicity due to the use of aminoglycosides can done anamnesis For know development And symptom early stages of the disease and supporting examinations to strengthen the patient's diagnosis.
Anamnesis
On anamnesis obtained voice ringing Which can happen is lost arise on during therapy or even become intense and persistent when therapy is stopped. Hearing loss may be asymptomatic and then become apparent after it interferes with conversational frequency. This becomes more severe if the drug is continued. In topical use ear Which contain aminoglycosides, decline hearing unilateral more likely to occur and symptoms This is not as severe as the manifestations of ototoxicity. vestibular in the ear.
Drugs that affect balance function (vestibular) will cause balance disorders with symptoms of lightheadedness and when looking at distant objects, the objects will appear to jump when the head is moved (oscilopsia) 32,33 .
Inspection
If aminoglycoside administration is planned for a patient, the patient's cochlear function must be examined. The examinations performed include pure tone audiometry, otoacoustic emission (OAE), vestibular function tests and brainstem evoked response audiometry (BERA) 41 . The examinations are performed primarily on patients at high risk and patients whose work is severely disrupted if there is a decrease in inner ear function 31,32 . Efforts to detect aminoglycoside ototoxicity early very important so that damage more carry on can prevented For kindness sufferer
32 .
Tone audiometry pure
Aminoglycosides impair hearing at high frequencies at the start of treatment, so it is advisable to perform a pure tone audiometry examination as a baseline at frequencies of 500 Hz, 1 kHz, 2 kHz, 4 kHz, 6 kHz and 8 kHz before starting treatment until 2 Sunday First therapy executed. Monitoring disturbance hearing performed during therapy, namely every week until 6 months after therapy is stopped 31,32,38 . Audiometry tone pure base very needed before giving aminoglycosides, especially in elderly patients who may already be suffering from a previous high frequency hearing loss condition 9 .
The hearing loss that occurs is sensorineural, namely early detection of aminoglycoside ototoxicity will result in an increase in hearing threshold of 15 dB or more at frequencies of 6 kHz and 8 kHz compared to previous pure tone audiometry, either unilateral or bilateral. This can occur 5-7 weeks from the start of therapy with aminoglycosides 32 . High frequency pure tone audiometry above 8 kHz has been shown to detect aminoglycoside ototoxicity earlier, but this tool requires frequency calibration Which regular And earphone Which special so that No Lots House Sick which has this facility 8.15
Criteria used by the American Speech Language Hearing Association (ASHA) in determine suspicion ototoxicity on use aminoglycoside There are three, firstly if there is an increase in the hearing threshold of 20 dB at one frequency, secondly an increase in the hearing threshold of 10 dB at two adjacent frequencies and finally there is a loss of response at three frequencies 49 .
OAE ( Otoacoustic Emission )
Otoacoustic emissions (OAEs) are the acoustic product of the movement of the outer hair cells of the cochlea. Otoacoustic emissions are more sensitive in detecting auditory dysfunction than audiometry tone pure frequency tall during therapy. There is two type OAE namely transient evoked otoacoustic emission (TEOAE) and distortion product otoacoustic emission (DPOAE). Distortion product otoacoustic emission is more sensitive than TEOAE, because DPOAE can detect small lesions along the organ of Corti or detect changes in outer hair cell activity before the lesion is large enough to be detected by audiometry15,38,49 . This test is relatively affordable, fast, objective, practical and does not require a soundproof room, making this test very useful, even in detect ototoxicity on patient Which No can give response subjective and reliable 38 .
Test Function Vestibular
Sensory input from the vestibular terminal organs, visual system, somatosensory and proprioceptive systems integrated on the stem brain, cerebellum and sometimes influenced by the cerebral cortex. Neurons in the vestibular nuclei form the vestibulospinal tract and the vestibulocerebellar tract. The connections between the vestibular and oculomotor nuclei are part of the medial longitudinal fasciculus, forming the anatomical basis of the vestibulo-ocular reflex. 42. Various vestibular function tests that can be performed directly ( bedside ) during drug administration are the oscilopsia test (dynamic visual field changes during active head movements), the head shake test and the Halmagyi test ( head thrust ) 39. The oscilopsia test (dynamic visual aquity testing) is performed by asking the patient to read the bottom line of an S- nellen board placed 20 feet away during rest time, then the patient's head is moved and the patient is again asked to read the bottom line of the S -nellen board . If there is a decrease in visual ability of more than 2 lines, it indicates significant bilateral vestibular disorders and this is typical of ototoxicity. 38,39,42 .
Inspection head shake is test Which sensitive to lesi vestibular unilateral. Head shake nystagmus is response involuntary Which useful For distinguish psychogenic dizziness from peripheral vestibular dysfunction. The patient's head is moved horizontally with fast, after that observed does nystagmus occur? or no. The slow phase occurs towards the lesion while The fast phase occurs away from the lesion 38. The head thrust maneuver is performed by lowering the patient's head 30 degrees, then the patient turn around to lateral 15-30 degrees, but eye still focus to target center (eg to nose examiner). Head sufferer moved return to center, eye still focus on the central target. Note whether there is a saccadic movement in the patient's eyes due to lack of visual fixation during the examination. Decreased visual fixation is associated with the decline function canal semicircular ipsilateral (side lesion)
31,49,50 .
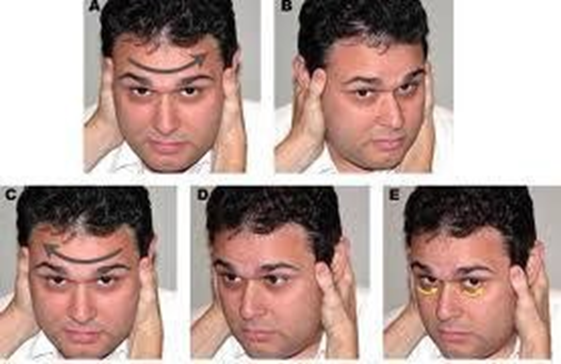
Figure 7. A. The patient's head is lowered 30 0. B. The patient's head is turned to the side. lateral not enough from 30 0 in a way fast with eye sufferer focus to nose examiner. Head sufferer moved to middle return. D. Action on B repeated to contralateral direction quickly. E. Note the saccadic movements that occur 50 .
BERA (Brainstem Evoked Response Auditory)
Some cases have found that toxicity affects the auditory nerve components without damaging the cochlear hair cells. This is known as auditory neuropathy. The changes that occur are significant changes in pure tone audiometry with normal or pass OAE results . The best examination in monitoring toxic effects on the Nervus Auditory is with BERA. Damage Which happen on Nerve Auditory or brainstem is indicated by increased latency on the BERA wave. This examination needs to be done if there is an indication 38 .
Therapy
Decrease hearing sensorineural Which permanent can overcome with tool hearing aids or cochlear implants. Monitoring of hearing function should be carried out during therapy until a number of month after caught effect ototoxic from aminoglycoside. Vestibular toxicity treated with rehabilitation vestibular Which speed up compensation vestibular. Function vestibular can return until 12 months after vestibulotoxicity occurs 16 .
Prevention
Substitute aminoglycosides with other types of antibiotics as soon as early symptoms of ototoxicity are observed.
Antioxidants
The mechanism of minimizing cell death by administering antioxidants begins with the process of preventing aminoglycosides from becoming a cytotoxin that causes mitochondrial dysfunction and reducing ROS (reactive oxygen species) levels so that they are ultimately able to minimize cell death 9 . Examples of antioxidants include:
Vitamin B, vitamins C, and vitamin E,
N-acetylcysteine
Sodium thiosulfate 46
Dosage adjustments especially for patients with renal impairment. In patients with renal impairment, the maintenance dose of aminoglycosides is half the normal dose 33,35 .
e. When using ear drops containing aminoglycosides, the following should be kept in mind, namely that the use of ear drops should be short-term (less than 7 days) or stopped once the otorrhea stops, regular monitoring of hearing and vestibular function and prioritizing topical drugs that do not cause ototoxicity, for example fluoroquinolones 40 .
Conclusion
Ototoxicity aminoglycoside is decline function And damage mobile in inner ear, in this case the cochlea, vestibule or vestibulocochlear nerve, caused by the use of aminoglycosides either systemically or topically
Symptoms of cochlear ototoxicity include tinnitus and sensorineural hearing loss in second ear or One ear. Decrease hearing will about frequency high above formerly before about frequency conversation. Symptom ototoxicity on vestibular is characterized by balance disorders or oscilopsia.
Early detection of ototoxicity includes anamnesis and examination, both pure tone audiometry, otoaccoustic emission and test vestibular function. Early detection of ototoxicity may find a 15 dB or greater increase in hearing thresholds at 6 kHz and 8 kHz, either unilateral or bilateral, usually occurring 5-7 weeks after initiation of aminoglycoside therapy. Early detection is essential in aminoglycoside ototoxicity so that further damage to the inner ear can be prevented. Aminoglycoside ototoxic therapy includes hearing aids or cochlear implants and rehabilitation vestibular.
REFERENCE
Schuman RM. Ototoxicity. In Bailey BJ. Head & Neck Surgery - Otolaryngology, 4th Edition. 2006 Lippincott Williams & Wilkins. Chapter 148. p645.
Bro, VHS And Bro, SS 1991 . Aminoglycosides in S Bro, R. Dear Mr. Setiabudi, U. Sjamsudin, Z. S. Bustami: Pharmacology And Therapy, edition 3. Part Pharmacology Faculty of Medicine, University of Indonesia, Jakarta, pages 599-614.
Sheikh A, Bint-e-Zainab, Shabbir K, Imtiaz A. Structure and Physiology of Human Ear Involved in Hearing. Intech. 2022;
Neng L, Shi X. Vascular pathology and hearing disorders. Curr Opin Physiol [Internet]. 2020;18:79–84. Available from: https://doi.org/10.1016/j.cophys.2020.09.004
Nyberg S, Joan Abbott N, Shi X, Steyger PS, Dabdoub A. Delivery of therapeutics to the inner ear: The challenge of the blood-labyrinth barrier. Sci Trans Med. 2019;11(482):1–12.
Alshuaib WB, Al-Kandari JM, Hasan SM. Classification of Hearing Loss. Intech. 2016;29– 37.
Mudd PA. Inner Ears, Ototoxicity. Article in medscape emdicine. 2008. Available from : http:// emedicine.medscape. com/article/857679- overview
The Great Hall S, Mantadakis E, Mavros M N, Ammari C, Phalagas ME. Pharmacological considerations for the proper clinical use of aminoglycosides. Drugs 2011; 71 (17):2277- 94.
Blackley BW. Intratympanic gentamicin in the treatment of meniere's disease. In: Roland PS, Rutka JA, eds. Ototoxicity. 1st ed. London: BC Decker Inc; 2004. p. 191-5.
Brunton, L.L.; Hilal-Dandan, R.; Knollmann, BC Goodman & Gilman's the Pharmacological Basis of Therapeutics, 13th ed.; McGraw-Hill Education: New York, NY, USA, 2018.
Cox, G.; Ejim, L.; Stogios, P.J.; Koteva, K.; Bordeleau, E.; Evdokimova, E.; Sieron, AO; Savchenko, A.; Serio, AW; Krause, K.M.; et al. Plazomicin Retains Antibiotic Activity against Most Aminoglycoside Modifying Enzymes. ACS Infect. Dis. 2018, 4, 980–987.
Kearns, G.L.; Abdel-Rahman, SM; Alander, SW; Blowey, D.L.; Leeder, J.S.; Kauffman, RE Developmental Pharmacology—Drug Disposition, Action, and Therapy in Infants and Children. N. Engl. J. Med. 2003, 349, 1157–1167
Chang KW. Ototoxicity. In: Johnson JT, Rosen CA, Newlands S, Amin M, Branstetter B, Casselbrant M, et al, eds. Bailey's head and neck surgery–otolaryngology. 5th ed. Vol 2. Philadelphia: Lippincot Williams & Wilkins; 2014. p. 2542-8.
Brandt T et al, 2003. Vertigo and Dizziness; Common Complaints. London.Springer ; pp. 127
Brandt T et al, 2005. Vertigo: It's Multisensory Syndromes. 2nd edition. London.Springer;
pp. 355- 358
Chambers, HF 2001. Antimicrobial agents in Gilman, AG, JG Hardman, LE Limbird (editors): Goodman & Gilman's The Pharmacological Basis of Therapeutics, Tenth Ed. McGraw-Hill Medical Publishing Divisions, New York, pages 1219-1235
Roland PS, Pawlowski KS. Ototoxicity. In: Wackym PA, Snow JBS, eds. Ballenger's otorhinolaryngology head and neck surgery. 17th ed. Connecticut: BC decker Inc; 2009. p. 273-6.
Faibanks DNF. Antimicrobial Therapy in Otolaryngology-Head and Neck Surgery. 13th edition. 2007. American Academy of Otolaryngology-Head and Neck Surgery Foundation, Inc.ChV,p73.
Schacht J. Mechanisms for aminoglycoside ototoxicity: basic science research. In: Roland PS, Rutka JA, eds. Ototoxicity. 1st ed. London: BC Decker Inc; 2004. p. 93-8.
Alharazneh, A., Luke, L., Huth, M., Monfared, A., Steyger, P. S., Cheng, A. G., & Richie,
A. J. (2011). Functional hair cell mechan- otransducer channels are required for aminoglycoside auto-toxicity. PLOS ONE, 6(7), e22347. https://doi.org/10.1371/ journal.pone.0022347
Marcotti, W., van Netten, S. M., & Kros, C. J. (2005). The amino- glycoside antibiotic dihydrostreptomycin rapidly enters mouse outer hair cells through the mechano- electrical transducer channels. Journal of Physiology, 567(Pt. 2), 505–521. https://doi.org/ 10.1113/jphysiol.2005.085951
Stepanyan, R. S., Indzhykulian, A. A., Velez-Ortega, A. C., Boger, E. T., Steyger, P. S., Friedman, T.B., & Frolenkov, G.I. (2011). TRPA1-mediated accumulation of aminoglycosides in mouse cochlear outer hair cells. Journal of the Association for Research in Otolaryngology, 12(6), 729–740. https://doi.org/10.1007/s10162-011-0288-x
Hailey, D.W., Esterberg, R., Linbo, T.H., Rubel, E.W., & Raible, D.W. (2017). Fluorescent aminoglycosides reveal intracellular traffic- Fucking routes in mechanosensory hair cells. Journal of Clinical In- vestigation, 127(2), 472–486. https://doi.org/10.1172/JCI85052
Cross, C. J., & Steyger, P. S. (2019). Aminoglycoside- and cisplatin-induced ototoxicity: mechanisms and autoprotective strategies. Cold Spring Harbor Perspectives in Medicine,
9(11). https://doi.org/10.1101/cshperspect.a033548
Roland NJ, McRae RDR, Mccombe AW. Ototoxicity. In: Roland NJ, McRae RDR, Mccombe AW, eds. Key topics in otolaryngology and head and neck surgery. 2nd ed. Oxford: Bios scientific publishers Ltd; 2001. p. 229-30
Mylonas I. Antibiotic chemotherapy during pregnancy and lactation period: aspects for consideration. Archieve Gynecology Obstetrics 2011: 287:7-18.
Turnidge, J. Pharmacodynamics and dosage of aminoglycosides. Infect Dis C/in N Am 2003; 17 : 503-528
Masjhoer, M. 1990. Effect Side Antibiotic, S. Suryawati, E. Kristin, Mustafa, B. Santosa
: Selection and Usage Antibiotics in Clinic Foundation Jasmine of the Archipelago. Yogyakarta, pages 60-63.
Lopez-Novoa, JM, Quiros, Y., Vicente, L., Moreales, AI, Lopez-Hernandez, FJ 2011. New insights into the mechanism of aminoglycoside nephrotoxicity: an integrative point of view. Kidney International, 2011; 79: 33-45
Mingeot-Leclerq, M., Tulkens, P.M., 1999. Aminoglycosides: Nephrotoxicily. Antimicrobial Agents & Chemotherapy, 1999; 43 (5): 10003-12
ElMouedden, M.,Laurent, G.,Mingeot- Leclercq,MP, Taper,HS, Cumps, J., and Tulkens, PM Apoptosis in Renal Proximal Tubules of Rats Treated with Low Dose of Aminoglycosides. Antimicrobial Agents and Chemotherapy (2000); 44(3): 665-675
Roland NJ, McRae RDR, Mccombe AW. Ototoxicity. In: Roland NJ, McRae RDR, Mccombe AW, eds. Key topics in otolaryngology and head and neck surgery. 2nd ed. Oxford: Bios scientific publishers Ltd; 2001. p. 229-30.
Iurato S. Ototoxicity. In: Europe manual of medicine in otorhinolaryngology-head and neck surgery. 1st ed. Berlin: Springer; 2010. p. 129-30.
Tange RA. Ototoxicity. In: Dhingra PL, ed. Diseases of ear, nose and throat. 4th ed. India: Elsevier; 2007. p. 34-5.
Fairbanks DNF. Ototoxicity, prevention and monitoring. In: Fairbanks DNF, ed. Pocket guide to antimicrobial therapy in otolaryngology – head and neck surgery. 13th ed. Alexandria: American Academy of Otolaryngology-Neck Surgery Foundation; 2007. p. 73- 6.
Al-Malky G, Suri R, Dawson SJ, Sirimanna T, Kemp D. Aminoglycoside antibiotics cochleotoxicity in pediatric cyctic fibrosis (cf) patients: a study using extended high-frequency audiometry and distortion product autoacoustic emissions. International Journal of Audiology 2011; 50:112-22.
Schacht J. Mechanisms for aminoglycoside ototoxicity: basic science research. In: Roland PS, Rutka JA, eds. Ototoxicity. 1st ed. London: BC Decker Inc; 2004. p. 93-8.
Mylonas I. Antibiotic chemotherapy during pregnancy and lactation period: aspects for consideration. Archieve Gynecology Obstetrics 2011: 287:7-18.
O'leary S. Ototoxicity. In: Gleeson M, Browning G, Burha MJ, Clarke R, Hibbert J, Jones NS, et al, eds. Scott-brown's otorhinolaryngology head & neck surgery. 7th ed. London: Edward Arnold Ltd; 2008. p. 3567-73.
Zarandy MM, Rutka J. Ototoxicity. In: Zarandy MM, Rutka J, eds. Diseases of the inner ear: a clinical, radiological & pathologic atlas. 1st ed. Berlin: Springer; 2010. p. 85-8.
Probst R. Inner ear and retrocochlear disorders. In: Probst R, Grevers G, Iro H, eds. Basic otorhinolaryngology, a step-by-step learning guide. New York: Thieme; 2006. p. 263-4.
Shin JJ, Lin MY, Rauch SD. Ototopical neomycin: impact on post- treatment hearing. In: Shin JJ, Hartnick CJ, Randolph GW, eds. Evidence-based otolaryngology. 1st ed. New York: Springer; 2008. p. 259-61.
Kisilevsky VE, Tomlinson RD, Ranalli PJ, Pre-Paging N. Monitoring vestibular toxicity. In: Roland PS, Rutka JA, eds. Ototoxicity. 1st ed. London: BC Decker Inc; 2004: p. 161-8.
Liu H, Ding D, Jiang H, Wu X, Salvi R, Sun H. Ototoxic destruction by co-administration of kanamycin and ethacrynic AC ID in rats. Journal of Zhejiang University-Science b (biomedicine & biotechnology) 2011; 12(10):853-61.
Shen Z, Zheng J, Peng G, Zhang T, Gong S, Zhu Y, et al. Frequency and spectrum of mitochondria 12S rRNA variants in 440 Han Chinese hearing impaired pediatric subjects from two otology clinics. Journal of Translational Medicine 2011; 9:15-21.
Van with water TR, Rybak LP. Ototoxic damage to hearing: autoprotective therapies. In: Roland PS, Rutka JA, eds. Ototoxicity. 1st ed. London: BC Decker Inc; 2004. p. 170-8.
Money Q, Steyger PS. Trafficking of systemic fluorescent gentamicin into the cochlea and hair cells. Journal of the Association for Research in Otolaryngology 2009; 10:205-19.
Roland PS, Wright CG. Topical aminoglycoside cochlear ototoxicity. In: Roland PS, Rutka JA, eds. Ototoxicity. 1st ed. London: BC Decker Inc; 2004. p. 114-9.
Prepageran N, Kisilevsky V, Rutka JA. Topical aminoglycoside vestibular toxicity. In: Roland PS, Rutka JA, eds. Ototoxicity. 1st ed. London: BC Decker Inc; 2004. p. 121-6.
Campbell KCM. Audiologic monitoring for ototoxicity. In: Roland PS, Rutka JA, eds. Ototoxicity. 1st ed. London: BC Decker Inc; 2004. p. 153-7.
Dhillon RS, East CA. Disorders of balance. In: Marks S, ed. Ear, nose and throat and head and neck surgery. 2nd edition. United Kingdom: Churchill Livingstone; 2000. p. 20-2.
Comments