DISTURBANCE HEARING ON CONGENITAL RUBELLA SYNDROME
I Made Nudi Arthana
Congenital Rubella Syndrome (CRS) is a collection of symptoms consisting of hearing loss, cataracts (clouding of the eye lens), congenital heart disease, and developmental delays. development, including delay talk And disability intellectual. Congenital rubella syndrome caused by rubella virus infection in the fetus during pregnancy due to the mother not having immunity to the rubella virus. A child may exhibit one or more symptom SRK with symptom most frequent is disturbance hearing. 1 If infection virus Rubella occurs in pregnancy, especially the first trimester often causes Congenital Rubella Syndrome. CRS causes abortion, stillbirth, premature birth and disability if the baby survives. The most common congenital defects are sensorineural deafness, eye damage such as cataracts, cardiovascular disorders, and mental retardation. 2-11
LITERATURE REVIEW
Embryology, Anatomy And Physiology Hearing
Embryology Ear
The development of the head and neck structures of mammals is the result of soft tissue differentiation from mammalian embryo, where the head and neck structures originate from soft tissue in the pharyngeal apparatus area of the embryo. 11 The development of the pharyngeal apparatus of the embryo forms three components, namely the branchial arch (pharyngeal), branchial pouch and branchial cleft, where the branchial arch is the main element where the structures of the mesoderm layer of the embryo develop such as muscle tissue, blood vessel elements and neural crest cells which will later form bone tissue and nerve tissue. Therefore, if there is a developmental disorder in the branchial arch, it will cause congenital abnormalities in the structure of the head and neck. 11,12
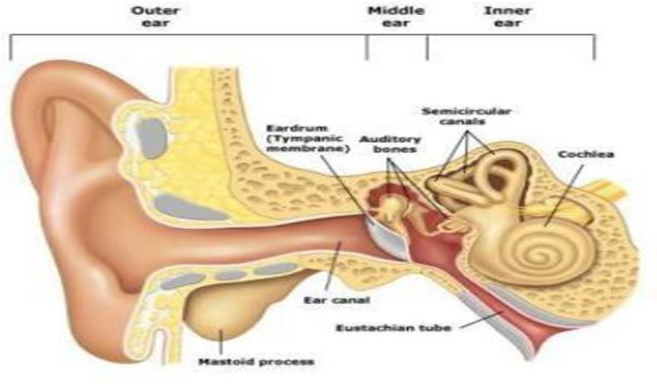
An important period for ear development is the 3rd week after fertilization, when the inner ear forms. moreover previously formed. Outer ear, middle And in originate from different embryology and their development can be disturbed at any level which can cause abnormalities that vary widely from from the light to the heavy one. 11
Auditory development is closely related to brain development. Neurons in cortex section experience maturation in time 3 year First life And in time The first 12 months of life see very rapid brain development. The tissues in the head and neck originate from 3 layer embryo, namely endoderm, mesoderm, And ectoderm. 12 Development prenatal is divided into several separate periods. The first period begins from the time of implantation of the blastocyst into the in wall uterus until circulation intraembryonic start formed, during This short period (about 21 days) the three layers of the embryo, namely the endoderm, mesoderm, and ectoderm develop into a flat, elongated plate containing the notochord. Structure like stem This originate from layer ectoderm And elongated throughout embryonic disc (embryo piece) starting from the buccopharyngeal membrane to the cloacal membrane , where the layer ectoderm And layer endoderm meet. Period second which is ongoing during 35 day (end) Sunday 8th) named period embryonic. During period This happen growth Which fast And differentiation level mobile so that on moment day 56th all system main And organ has formed, And embryo own form Which can stated as man. Time The remaining 7 months of gestation are called the fetal period, where rapid growth is only marked by changes in shape and position between one structure and another and no new cell differentiation is found as occurs in the embryonic period. 13
Anatomy Inner Ear
The inner ear or labyrinth consists of the bony labyrinth and the membranous labyrinth. part bone consists of from canal semicircular, vestibule And cochlea, whereas The membranous labyrinth is located within the bony labyrinth and consists of the semicircular canals, utricle, saccule and cochlea. 14
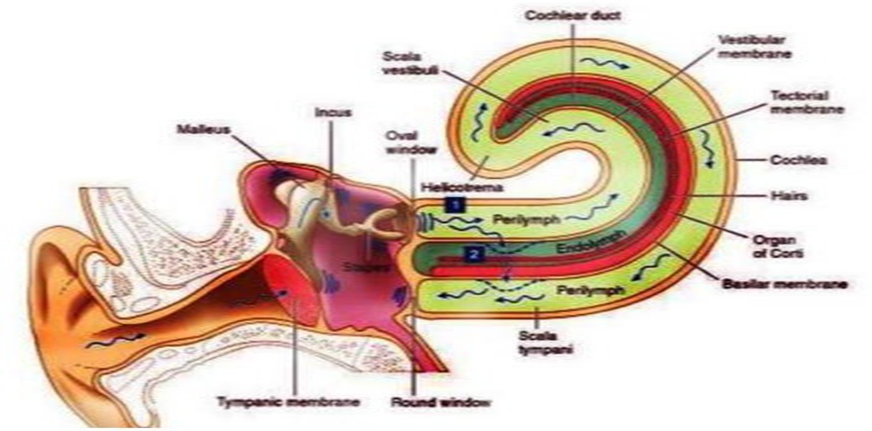
The cochlea is a bony canal that resembles a snail shell and is coiled 2½ turns, approximately 35 mm long with a center called the modiolus and is also place the exit laminate spiral. From laminate spiral stick out to wall outside cochlea a basilar membrane. At the attachment point of the basilar membrane to the outer wall of the cochlea there is a thickening of the periosteum known as the spiral ligament. In addition there is also membrane vestibular (Reissner) Which stretch throughout cochlea from laminate spiralis to the outer wall. These two membranes will divide the bony cochlear duct into three parts, namely the upper chamber (scala vestibuli), the middle chamber (ductus cochlearis/scala media), and the lower chamber called the scala tympani. The scala vestibuli and the cochlear duct are separated by the vestibular membrane (Reissner). The cochlear duct and the scala tympani are separated by the membrane basilar. Scale vestibule And scale timpani contain perilymph And the wall consists of network tie that coated by one layer cell flat, namely cell mesenchyme, which is fused with the periosteum on the outside. The vestibular scale is connected to the vestibular perilymph space and will reach the inner surface of the oval window. The tympani scale extends laterally to the round window which separates it from the tympanic space. At the apex of the cochlea, the vestibular and tympani scales will meet through a narrow channel called the helicotrema. 15
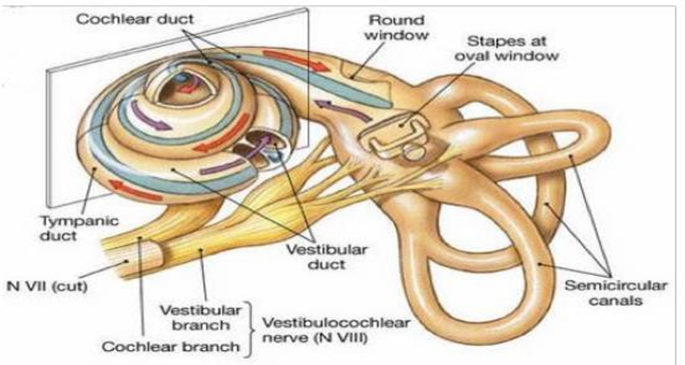
Picture 1.2 Cochlea And anatomy ear 15
The organ of Corti is located above the basilar membrane which contains important organs for the peripheral nervous mechanism of hearing, consisting of three main parts, namely supporting cells, hair cells and a gelatinous layer connecting the tectorial membrane. 16
Fluid perilymph has composition ions similar to fluid cerebrospinal fluid (CSF) and is also similar to extracellular fluid, with high sodium (Na+) and low potassium (K+) concentrations. The perilymph fluid in the scala vestibuli originates from blood plasma found in the hematoperilymphatic barrier, while the perilymph fluid in the tympani scale comes from CSF. 14
Endolymph fluid is a fluid that has almost the same ion composition as intracellular fluid and fills the auditory membrane and vestibular labyrinth. Endolymph is formed by cells Secret on stripe vascular and by dark cells in near end from Christ ampullary in the semicircular ducts and the walls of the utricle. Endolymph is absorbed in the endolymphatic sac. The composition of this fluid is high in potassium (K+) and low in sodium (Na+). The concentration potassium 144 mEq/L and sodium 13 mEq/L. The media scale has resting potential of about 80 mV decreasing from base to apex. This endocochlear potential is generated by the stria vascularis in the lateral wall of the cochlea. 16,17
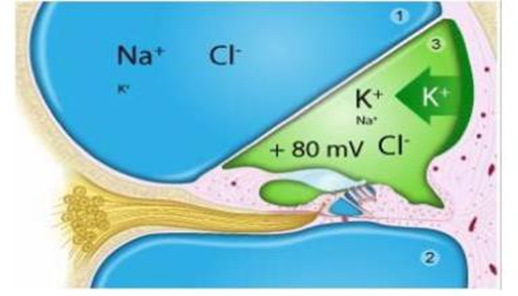
Picture 3 Composition Fluid Cochlea 15
Membrane basilaris is structure fibrous Which layered from laminate spiral pars osseous to ligament spiral. Elasticity membrane basilaris varies in throughout cochlea from stiffness and its width. Membrane basilaris looks rigid And narrow in area base cochlea. On area This is an area that is sensitive to high frequencies. While the other end of the membrane, namely at the apex of the cochlea, appears more flexible and wide and is most sensitive to low frequencies. 14
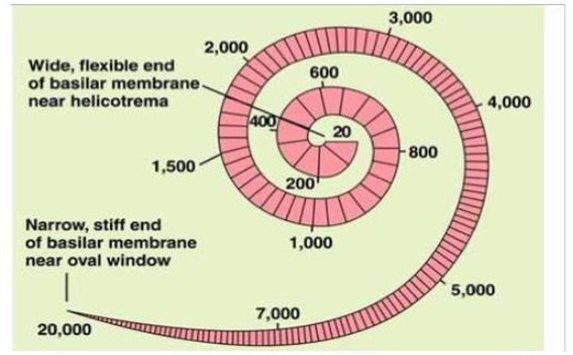
Picture 4 Width Membrane Basilaris from Basal to Apex. 15
The organ of Corti houses the auditory sensory cells. The organ of Corti is located along the basilar membrane, and projects from the base to the apex of the cochlea. The size of the organ of Corti varies gradually from the base of the cochlea to the apex of the cochlea. The organ of Corti consists of supporting cells And cells hair. Cell hair is cell sensory Which produce impulse nerves in response to vibrations of the basilar membrane. In the organ of Corti there is 1 row of inner hair cells and 3 to 5 rows of outer hair cells. There are about 3500 inner hair cells and 12000 outer hair cells. The cells - cell it differs morphologically, the shape of cell deep hair like bottle And the nerve endings are cup-shaped which covers them, while the shape of the cell The outer hairs are cylindrical and their nerve endings are only at the base of the cells which lie freely in the perilymph in the organ of Corti. 16
Cell hair in And outside this hold role important on change energy mechanics become energy electricity. Function cell hair in as mechanoreceptor main Which sends nerve signals to the auditory neurons of the spiral ganglion and the hearing center, while the function outer hair cells are to increase or sharpen the peak of the traveling wave by increasing the activity of the basilar membrane at certain frequencies. This increase in movement is called the cochlear amplifier which gives the ear excellent ability to select frequencies, the ear becomes sensitive and able to detect weak sounds. The tip of Hair cells contain actin fiber bundles that form tubes and enter the cuticular layer. (stereocilia). Stereocilia from cell hair in No attached on membrane tectorial and shaped letter U whereas stereocilia from cell hair outside strong attached on membrane upper tectorial and shaped like the letter W. 18
GJB2 (Connexin 26) is one of the main proteins that plays a role in homeostasis. in in cochlea in ear in. Connexin 26 is a group protein in the gap junction which plays an important role in communication between various components of hair cells, regulation of electrolyte movement and electrolyte metabolism of hair cells. Connexin 26 is expressed in non-sensory epithelium (interdental cells of the spiral limbus, supporting cells, inner and outer sulcus cells, and spiral ligament cells) and connective tissue cells (fibrocytes of the spiral ligament and spiral limbus, intermediate and basal cells in the stria vascularis). Six Connexin 26s form connexons, and each connexon connects to each other to form a gap junction. GJB2 gene mutations are the main cause of deafness that occurs in ear part in so that cause deaf sensorineural . Around 80% from deaf prelingual is genetic, most often autosomal recessive and nonsyndromic. The most common cause from disturbance recessive nonsyndromic hearing loss autosome severe to severe in most of the population is the GJB2 mutation. 14
Physiology Hearing
Sound vibrations are captured by the auricle which are transmitted to the ear canal and hit the tympanic membrane so that the tympanic membrane vibrates. The amplitude of the vibration of the tympanic membrane is in accordance with the intensity of the sound. This vibration is transmitted to the auditory ossicles (malleus, incus, stapes) which are connected to each other. When the wave reaches the base of the stapes, it will vibrate the fenestra ovale which is the attachment of the base of the stapes to the cochlea. Then the vibration will push the perilymph fluid in the vestibular scale in the cochlea in the internal auricle. The presence of pressure on the perilymph fluid in the vestibular scale will increase the pressure in the vestibular scale. This pressure will then be transmitted to the tympanic scale through the helicotrema. The fluid in the tympanic scale is also pressed. This causes pressure on scale timpani increase, Then pressure fluid timpani will push the fenestra rotundum located on the lateral side of the scala tympani towards the lateral side. Due to the compliance/flexibility of the fenestra rotundum, after being pushed laterally, it will return to its original position so that the pressure will be reflected back to the scala tympani, helicotrema, then to the scala vestibuli, and so on. The vibrations are transmitted through the Reissner membrane which pushes the endolymph and basilar membrane downward. The peak of the wave that travels along the basilar membrane which is 35 mm long is determined by the frequency wave voice. Membrane basilaris Which located near ear middle more short and stiff, will vibrate when there is a vibration with a low tone. This can be likened to a short guitar string and tense, will resonate with high pitch. Vibration which is high-pitched in the perilymph of the vestibular scale will cross the basal basilar membrane. Conversely, low tones will vibrate the basilar membrane in the apex area. These vibrations will then descend into the perilymph of the tympani scale, then exit through the foramen rotundum to the middle ear to be dampened. 19
The basilar membrane is a membrane that separates the scala tympani from the scala media. The upward movement of the basilar membrane will bend the stereocilia towards the stereocilia. more tall on phase depolarization result in the occurrence stretching on fiber tip link at the top of the stereocilia. When the tip link stretches, it immediately opens the mechanoelectric transduction (MET) channel on the stereocilia membrane and causes K+ current flow into the sensory cell. Potassium flow occurs because there is a difference in endocochlear potential +80 mV and negative intracellular potential in the hair cell, inner hair cell -40 mV and outer hair cell -70 mV. This results in intracellular depolarization which causes cations including potassium and calcium to flow into the hair cell. The entry of K+ ions will change the electrical potential in the hair cell and depolarize the cell, ultimately the hair cell shortens by affecting the outer hair cell motor or prestin. 14,16
When membrane basilaris move down, stereocilia bend to direction stereocilia The shortest time in the hyperpolarization phase results in relaxation of the tip link fibers at the top of the stereocilia, so the MET channel will close. If the stereocilia are perpendicular, opening the MET channel will have no effect. Tip this link like elastic channels that can control the opening and closing of the MET channels. K+ ions exit from the outer hair cells into the extracellular space around the outer hair cells and then enter the supporting cells.
Sound stimuli are converted into vibrations of the basilar membrane, and lead to the opening and closing of the MET channels in the stereocilia, which then produce an electrochemical response and will finally present the sound to the auditory nerve. 14,16
The cochlear nerve fibers run to the dorsal and ventral cochlear nuclei. Most of the core fibers cross the midline and run up to the contralateral inferior colliculus, but some fibers continue to run ipsilaterally. The next crossing is at the lateral lemniscus and the inferior colliculus. From the inferior colliculus the auditory pathway continues to the geniculate body and then to the auditory cortex in the temporal lobe. 16
Picture 5 Physiology Hearing. 15
Syndrome Rubella Congenital
Definition
Syndrome Rubella Congenital (SRK) is disease on baby by Because infection maternal rubella virus infection during pregnancy. When rubella infection occurs during early pregnancy, serious consequences such as abortion, IUFD and severe birth defects in the baby can occur. The risk of congenital infection and disability is highest during the first 12 weeks of pregnancy and decreases after Sunday the 12th pregnancy; rare defect happen after infection on sunday 20th (or later) pregnancy. 20
SRK is combination a number of abnormality physical develop in baby as a result infection virus rubella mother Which to be continued in fetus. Name other SRK is Fetal Rubella Syndrome. The most common congenital defects are sensorineural deafness, eye damage such as cataracts, cardiovascular disorders, and mental retardation. 20
Epidemiology
SRK First time reported on year 1941 by Norman Greg a Australian eye specialist who found congenital cataracts in 78 babies whose mothers had rubella infection early in pregnancy. According to WHO data, around 236,000 cases of CRS occur each year in developing countries and increase 10-fold during epidemics. 20
On year 1969, vaccine rubella life licensed in American Union. Objective program vaccination is the elimination of rubella and continues to be the prevention of congenital rubella infection, including SRK. On year 2004 elimination rubella has achieved in American Union. During 2005–2015, the number of reported CRS cases in the United States decreased to <2/100,000 live births, 1.7 in Israel, 1.5 in Singapore and 0.5 in Malaysia. In Indonesia, studies on rubella incidence have not been widely conducted. However, from This small study, it is estimated that the incidence of rubella infection is quite high. 21 Riskesdas 2011 data obtained ±400 cases of congenital rubella syndrome, while according to WHO in 2012 around 5000-10,000 babies were born with deafness per year. 20
Data WHO, case rubella in Asia Southeast on year 2017 as much as 4,386, down from 10,361 cases in 2016. 22 According to data Ministry Health Republic Indonesia, on year 2015 happen decline coverage immunization from year previously. 23 Cases rubella reported Still tall And is one of the public health problems that requires effective prevention efforts. Indonesia committed to achieve elimination measles And control rubella/SRK on year 2020 with one of strategy campaign vaccination on age 9-15 years since August 2017. 23
Etiology And Pathogenesis SRK
Rubella virus was first isolated in 1962 by Parkman and Weller. Rubella is an RNA virus belonging to the genus Rubivirus, family Togaviridae, with a single antigen type that cannot react cross-relationship with a number of other Togavirus groups. Rubella virus own 3 protein structural main that is 2 glycoprotein envelope, E1 And E2 And 1 nucleocapsid protein. In general morphology, virus rubella shaped round (spherical) with diameter 50–70 mm and has a dense nucleoprotein core, surrounded by two layers of lipid containing glycoproteins. E1 And E2. Virus rubella can be destroyed by proteinase, fat solvents, formalin, ultraviolet light, low pH, heat and amantadine but relatively susceptible to freezing, thawing or sonication. 2
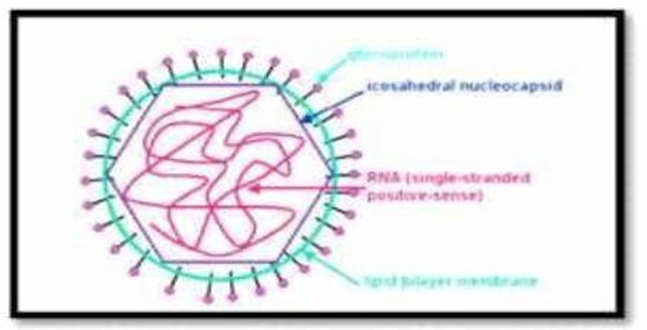
Picture 6 Virus Rubella. 20
Rubella virus consists of of two large structural subunits, one related with envelope virus and others related to nucleoprotein core Rubella virus consists of glycoprotein layer, fat and core with RNA. 20
The rubella virus is transmitted through respiration, namely through droplets released by the someone who is infected rubella, after exposed to droplets, this virus will undergo replication in nasopharynx And in area gland sap clear before reach organ target through Systemic circulation. Viremia occurs between the 5th and 7th day after exposure to rubella virus. In a closed room, rubella virus can be transmitted to anyone in the same room as the person. sufferer. Incubation period virus rubella range between 14–21 day. period transmission 1 week before and 4 days after the onset of the rash (rash). In this episode, the rubella virus is very contagious. 2
When infection virus rubella happen during beginning pregnancy, then serious risks more common are abortion, stillbirth and so on. The risk of congenital infection and defects increases during the first 12 weeks of pregnancy and decreases after pregnancy above 12 weeks with defects rarely occurring at 20 weeks of pregnancy. 24 If infection occurs in the first month of pregnancy, the risk of developing CRS as much as 43 percent. The risk increases to 51 percent if the infection occurs in the first 3 months of pregnancy, The risk decreases if the infection occurs after the first 3 months of pregnancy (23%). 24
Transplacental infection of the fetus in the womb occurs when viremia occurs. Rubella infection causes fetal damage because the division process is inhibited. In the pharyngeal secretions and urine of infants with CRS, there are large amounts of rubella virus that can infect if in direct contact. Viruses in baby body with SRK can last up to several months or less than 1 year after birth. 25
Damage fetus due to by various factor, for example by damage cell consequence rubella virus and the effects of cell division by the virus. Placental infection occurs during maternal viremia, causing focal areas of necrosis in the chorionic villi epithelium and capillary endothelial cells. These cells desquamate into the lumen of blood vessels, and rubella virus then enters the fetal circulation as emboli of infected endothelial cells. This in turn results in infection And damage fetal organs. During early pregnancy mechanisms The fetal defenses are not yet mature and the typical picture of embryopathy in early pregnancy is the occurrence of cellular necrosis without signs of inflammation. 26
Rubella virus-infected cells have a short lifespan. Infected fetal and infant organs own amount cell Which more low than baby Which Healthy. Virus rubella Also can trigger the occurrence damage with method apoptosis. If infection mother happen after first trimester pregnancy, frequency And the weight degrees damage fetus decrease drastic. Difference this happened because of the fetus protected by development response immune fetus, both humoral and cellular, and the presence of maternal antibodies that are passively transferred. 27
On infection rubella maternal, Which usually happen five until seven day after inoculation in the mother, the virus spreads throughout the placenta hematogenously, leading to congenital infection. Which potential in the fetus that currently develop. In infection maternal rubella with rash, the frequency of congenital infection is more than 80% during the first 12 weeks of pregnancy, about 54% at 13-14 weeks, and about 25% by the end of the second trimester. Any maternal rubella infection that occurs after 16 weeks of pregnancy, there is no risk of congenital rubella syndrome in the newborn. 28
Several studies have shown that the route of rubella virus infection is through systemic organs in the human fetus. This fact has been confirmed by immunohistochemical tests and direct detection of viral RNA in several organs. The main histopathological changes were observed in the liver. The embryonic liver has a very important role in the process of hematopoiesis besides the bone marrow. bone. Findings of viral antigen in glomerular and proximal tubular epithelial cells in the kidneys also showed excretion of the virus in the urine. 26
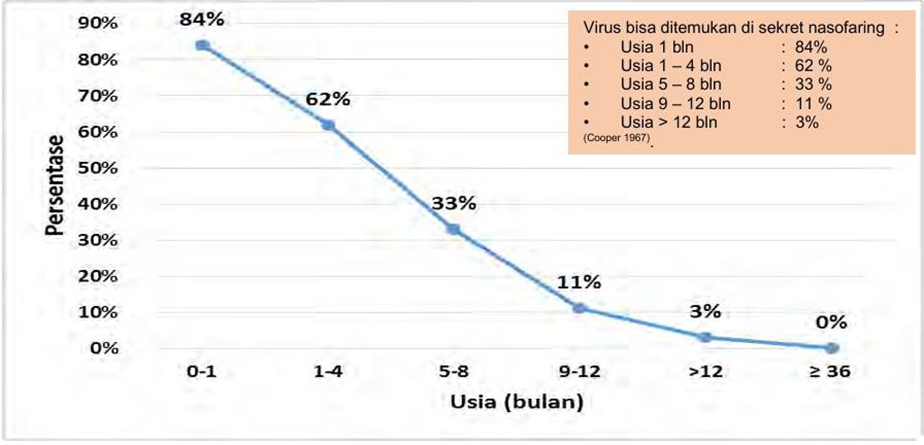
Rubella virus is transmitted through respiratory droplets when coughing or sneezing. Infants with CRS can still excrete rubella virus through urine and nasopharyngeal secretions until the age of 27 months, but most of it is gone before the age of 1 year. Virus can be found in secretions nasopharynx as much as 84% on baby with CRS on month First his life, then decreased to around 62% at age 1 – 4 months; 33% at the age of 5-8 months, 11% at the age of 9 – 12 months, and only around 3% in the second year of life
Manifestation Clinical
Rubella is disease infection Which 20–50% case among them nature asymptomatic. Rubella symptoms are almost similar to other diseases accompanied by rashes. Clinical symptoms to diagnose rubella virus infection in adults or during pregnancy are acute infections characterized by maculopapular rash, body temperature >37.2°C and arthralgia/arthritis, lymphadenopathy, and conjunctivitis. 26
If Rubella attacks a pregnant mother under three months of age, the infection can cause severe congenital abnormalities in the baby. According to Pumper and Yamashiroya, between 50% and 80% of fetuses exposed to the mother's Rubella virus can develop fetal infection before 8 weeks of gestation. Infection is less common after the 3rd trimester, namely 6-10%. Some organs that are very susceptible to disorders due to Rubella infection include the eyes, ears, heart, and central nervous system including the brain. The risk of congenital defects reaches almost 90% in infections with onset in the first trimester of pregnancy, then decreases to approximately 10-20% by the 16th week and is less common when Mother caught infection on age pregnancy after 20 week. Abnormalities congenital the effects of infection in pregnancy are related to disruption of the embryogenesis process in the first trimester. Infection intrauterine Which most general cause abnormality congenital covering TORCH (Toxoplasma gondii, Rubella, Cytomegalovirus, Herpes Simplex), as well as other causes, namely Treponema pallidum, Varicella zoster, Epstein Barr virus, Lymphocyte choriomeningitis virus, and West Nile virus.
SRK Which covering 4 defect main that is: 2
Disturbance hearing type sensorineural. arise when infection happen before age 8 weeks pregnant. This symptom may be the only symptom that occurs.
Disturbance heart covering PDA, VSD And stenosis pulmonary.
Disturbance eye : cataract And glaucoma. Disorder This seldom stand Alone.
Retardation mentally

Risk infection fetus diverse based on time the occurrence infection maternal. Infection occurs in 0–12 Sunday age pregnancy, so happen 80–90% risk infection fetus. Infection mother that happened before happen pregnancy No influence fetus. Infection mother on age pregnancy 15–30 Sunday risk infection fetus decrease that is 30% or 10–20%. Baby in diagnosis experiencing CRS when experiencing 2 symptom on criteria A or 1 criteria A And 1 criteria B, as following:3
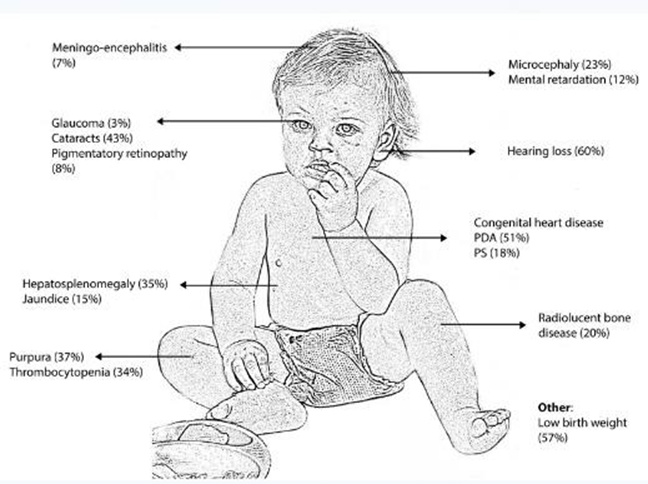
A. Cataracts, congenital glaucoma, congenital heart disease (most commonly PDA or peripheral pulmonary artery stenosis), hearing loss, retinal pigmentation. B. Purpura, splenomegaly, jaundice, microcephaly, mental retardation, meningoencephalitis and radiolucent bone disease (bones appear dark on x-ray). Some cases have only one symptom and hearing loss is the most common defect found in infants with CRS. Definition lost According to WHO, hearing is the limit of hearing ≥26 dB which is incurable and permanent. 20
Babies and children with hearing loss often show symptoms of delayed speech. talk (speech delay). No development ability speak And speaking is a sign that indicates hearing loss and needs to be evaluated. Development talk close the relation with stage development hear on baby, So hearing loss needs to be suspected if: 29
Age 12 month : Not yet can rambling (babbling) or copy sound
Age 18 month : No can to mention 1 say Which have meaning
Age 24 months : treasury say less than 10 say
Age 30 month : Not yet can string together 2 say Development auditory in accordance with age children, including: 29
Age 0-4 month : ability response auditory Still limited And nature reflex. Can asked whether the baby was startled by a loud noise or woke up while sleeping. The response was in the form of an auropalpebral reflex or a Moro reflex.
Ages 4-7 months respond to turning the head towards sounds located in the horizontal plane, although Not yet consistent. On age 7 month muscle neck Enough strong so that head can be rotated quickly towards the sound source.
Age 7-9 months can identify with right on the origin sound source and baby can turn the head firmly and quickly.
Age 9-13 months baby already have a great desire to seek sound source from above, and at 13 months of age is able to quickly localize sounds from all directions.
At the age of 2 years, the examiner must be more careful because the child will not react after several times receiving the same stimulus. This is because the child is able to estimate the source of the sound.
Inspection support
Inspection laboratory done For support infection diagnosis virus rubella and to status immunological. Because procedure isolation virus very long And expensive as well as response Host antibodies are very fast and specific, so serological examinations are more often performed. Examination materials to determine the presence of rubella virus infection can be taken from throat swabs, blood, urine and others. The following table which contains the types of examinations and specimens used to determine rubella virus infection. 2
Table. Type inspection & specimen For determine virus rubella
In general line big, inspection laboratory For determine infection virus rubella divided into 3, namely: 2
Isolation virus
Rubella virus can be isolated from nasal discharge, blood, smear throat, urine, and cerebrospinal fluid rubella sufferers. The virus can also be isolated from the pharynx 1 week before and up to 2 weeks after the appearance of the rash. Although this isolation method is a definitive diagnosis for rubella infection, it is rarely performed because the procedure complicated examination. Matter this causes method virus isolation No as method diagnostic routine. For isolation in a way primary specimen clinical, often using cell culture namely Vero; African green monkey kidney (AGMK) or with RK-13. Rubella virus can be found with Cytopathic effects (CPE).
Inspection serology
Inspection serological used For diagnose infection virus rubella congenital and postnatal (often done in children And person mature young) And For determine the immunological status against rubella. Examination of pregnant women who have had contact with rubella with sufferer rubella, requires effort diagnosis serologically right and careful. If sufferer show symptom clinical Which the more burdensome, so must be done immediately done inspection immunoassay enzyme (ELISA) against serum sufferer to determine existence IgM rubella-specific, Which can confirmed with inspect in the same way after 5 days later. Patients without clinical symptoms but diagnosed serologically are a problem special. They may are experiencing primary infection or re-infection because they have been vaccinated and have antibodies. Measurement rubella IgG levels with ELISA can also help differentiate between primary and reinfection.
In general specific, There is 5 objective inspection serological rubella, that is:
Help set diagnosis rubella congenital. In matter This done IgM immunoassay against rubella
Help set diagnosis rubella I on sufferers who suspected. To It is necessary to carry out IgM immunoassay on the patient
Examine mothers with a history of “rubellaform” rash in the past, before and in early pregnancy. Because this kind of skin rash can be caused by various other viruses
Monitoring Mother pregnant Which suspected infected rubella during pregnancy because Often the mother is exposed to the rubella virus at the beginning of her pregnancy (for example at the BKIA and Community Health Center)
Knowing the level of immunity of a person after vaccination. The presence of rubella IgG antibodies in serum the sufferer shows that sufferer said ever infected virus and maybe own immunity to virus rubella. Interpretation results IgM And IgG ELISA for rubella as test filter For pregnancy is as following: beforepregnancy, when positive There is protection (protection) And when negative means No given, early pregnancy (first trimester). IgG levels ≥15 IU/ml, are generally considered to be protective fetus against rubella. After vaccination; if positive means there is protection and if it is negative it means there is none.
Table. Interpretation results IgM And IgG ELISA For rubella
Inspection RNA
Types of examinations that can be performed to identify rubella virus RNA include :
Polymerase Chain Reaction (PCR): PCR is the most commonly used technique for detecting viral RNA. In the UK, PCR is used as a routine evaluation method for detecting rubella virus in clinical specimens. Detection of rubella RNA in amniotic fluid using RT-PCR has a sensitivity of 87–100%. Amniocentesis should done not enough from 8 Sunday after onset infection And after 15 weeks of conception. RT-PCR test using saliva samples is an alternative to serum which is often used for surveillance purposes.
Reverse Transcription-Loop-Mediated Isothermal Amplification (RT-LAMP) RT-LAMP is one type of examination to identify rubella virus RNA. In a study comparing the sensitivity between RT-LAMP, RT-PCR and virus isolation examinations conducted in Japan, it was found that the results were 77.8% for RT-LAMP, 66.7% For RT-PCR And 33.3% For isolation virus. Inspection RT-LAMP similar with inspection RT-PCR but results inspection in RT-LAMP can known by looking at the level of turbidity after incubation in a turbidimeter .
Disturbance Hearing on Syndrome Congenital Rubella
Sensory Neural Hearing Loss (SNHL) is the most common disorder of infection. congenital rubella (58%) and most often seen during infection rubella in the mother occurs in The first 16 weeks of pregnancy. The mechanism of hearing loss due to rubella is not fully understood, virus This causes damage cochlear And death cell directly in the organ of Corti and stria vascularis. 30 Hearing loss usually manifests in the first 6 – 12 months of life, although it can occur at birth. 31
Disturbance hearing due to there is a failure development system hearing loss with abnormalities occurring in the cochlea and auditory nerve. The virus causes direct damage to the cochlea, causing cell death in the organ of Corti and the stria vascularis. Rubella virus enters the inner ear through the blood supply of the stria vascularis. Other mechanisms may be caused due to hypoxia due to damage vascular endothelial damage. endothelium can be a source of embolism and cause thrombosis in small blood vessels. 32
Hearing loss is estimated to occur in around 80-96% of CRS patients and can occur unilaterally or bilaterally with varying degrees of severity. Rubella virus can directly affect cochlea by inducing apoptosis in the stria vascularis, cochlear duct and organ of Corti. The stria tissue can be infected and change the structure of the endolymph. Vasculitis occurs and directly damages the cochlear cells which interferes with myelination of the auditory nerve. 32
Diagnosis
Early diagnosis is important, so that early intervention can be performed. The diagnosis of CRS is established with 2 symptoms of criterion A (cataracts, congenital glaucoma, congenital heart disease such as patent ductus arteriosus or peripheral pulmonary artery stenosis, hearing loss, retinal pigmentation) or 1 criterion A with criterion B (purpura, splenomegaly, jaundice, microcephaly, mental retardation, meningoencephalitis, and radiolucent bone disease). The diagnosis is made clinically and supported by supporting examinations for virus isolation or serological examination. Examination materials to determine the presence of Rubella virus infection include throat swabs, blood, and others. To confirm suspected congenital rubella, maternal and neonatal specimens should be examined. If acute rubella is suspected in pregnant women, the method diagnosis most easy is test level serum mother to IgM rubella with EIA or IFA. RT-PCR for RNA rubella virus is done on liquid amnion almost 100% sensitive and specific and can also be performed on placenta and autopsy tissue. Congenitally infected neonates are IgM positive and excrete rubella in the urine for months to years. CRS is defined as combination Rubella specific IgM positive and clinically confirmed SRK. Sensitivity And specificity highest test IgM can be achieved with use µ-capture ELISA and by testing samples within 3 months of birth. In addition, monitoring of rubella-specific IgG may be helpful because persistent rubella-specific IgG after 4-6 months is highly indicative of congenital infection. When available, detection of viral RNA in urine and throat swabs by PCR provides a rapid and reliable diagnosis . 33
Diagnosis of SRK is confirmed by serological examination and virus isolation. Virus isolation through taking specimen nose, blood, throat, urine, And fluid cerebrospinal with reverse transcription polymerase chain reaction (RT-PCR). Serology test with Enzyme Linked Immunosorbent Assay (ELISA) for the diagnosis of CRS is more frequently used because it is widely available.
Development hearing started moment Still in content, baby prepared to respond to sounds at birth. The complex process of recognizing the mother's voice and distinguishing between sounds and noises can be seen in newborns. The baby's initial response to sound is a reflex (behavioral responses) such as the auropalpebral reflex (blinking), pulse heart increase, eyes widening (widen) eye), cessation (stop breastfeeding) and frowning or grimacing. 32
At the moment emission otoacoustics and brainstem evoked response audiometry (BERA) is a gold standard examination technique with the principle of fast, easy, non-invasive examination with a sensitivity approaching 100%. 34
Emission Otoacoustic
Otoacoustic emissions are low-intensity sounds produced by the outer hair cells of the cochlea and recorded in the external acoustic meatus either in the absence of acoustic stimulation (spontaneous emissions) or in response to acoustic stimulation (acoustic-evoked emissions). emissions) or stimulation electricity (electricity causes emission). Sound Which captured by cochlea very small range on 30 dB, However potential For heard. Emission otoacoustic embossed in a way spontaneous Because voice Which Already There is in cochlea in a way Keep going continuously circulate, but in general otoacoustic emissions are preceded by stimulation. Otoacoustic emissions are produced only when the organ of Corti is in a state close to normal, and the middle ear is functioning well . 35
This otoacoustic emission was first discovered by Gold in 1948 and introduced by David Kemp in 1978. In the otoacoustic emission examination, a certain sound stimulus is given through a mini loudspeaker located in an ear plug (insert probe). Which part outside coated rubber soft (probe tip). Microphone used For detect otoacoustic emissions, then convert them into electrical for easy processing. 35
Otoacoustic emissions are produced by the movement of the tympanic membrane which is transmitted to the cochlea through ear middle in a way spontaneous or use stimulus. To record otoacoustic emissions requires a healthy middle ear condition with good sound conduction. The cochlea does not significantly emit sound into the air in the tympanic cavity. In order for the movement of the membrane timpani efficient, more congested And A little air Which Can go out enter hole ear, then the ear canal must be closed. 35
The vibrations produced by the unique cochlear mechanism are known as the “cochlear amplifier” which causes the movement of the cells. outer hair in inner ear. Movements This can happen Good in a way spontaneous and also by stimulation sound from outside and is produced by active cell mechanisms. 35
Movement cell hair outside can was initiated by sound click with intensity currently or a combination Which in accordance from two tone, Then happen movement biomechanics from membrane basilaris resulting in intracochlear energy amplification and cochlear tuning. The movement of the outer hair cells generates mechanical energy in the cochlea which is amplified and exits through the middle ear system and tympanic membrane to the ear canal. 35
Results inspection easy read Because stated with criteria Pass (passed) or Refer (failed). Results Pass show condition cochlea Good; whereas results Refer It means presence of cochlear disorders. 35
Brainstem Evoked Response Audiometry (BERA)
Brainstem Evoked Response Audiometry (BERA) is a technique for measuring nerve activity or response to sound stimuli. The BERA examination was first reported by Sohmer And Feedback on year 1967, Which Then explained more details by Jewett and Wilson in 1971. BERA is an electrophysiological test that generates electrical potentials at various levels of the auditory system from the cochlea to the cortex. BERA is generated by acoustic stimuli (clicks or beeps) sent by an acoustic transducer in the form of earphones or headphones. 35
Brain Evoked Response Audiometry or BERA is a tool that can be used to detect early hearing loss, even since the baby was just born. Other terms that are often used are Brainstem Auditory Evoked Potential (BAEP) or Brainstem Auditory Evoked Response Audiometry (BAER). This tool effective to evaluate the auditory canal or organ from the periphery to the brain stem. 36
The use of the BERA test in the fields of audiology and neurology is very beneficial. And have mark objectivity Which tall when compared to with conventional audiology examination. Its easy use, non-invasive, and can be performed on comatose patients, makes this BERA examination widely used. 36
The BERA test can assess function hearing of uncooperative infants or children. Which cannot be checked by conventional means. Unlike audiometry, this tool can be used on both cooperative and uncooperative patients such as in newborns, young children, patients who are in a coma or stroke, it does not require an answer or response from the patient as in audiometry because the patient must press a button if they hear a sound stimulus. This tool also does not require a special soundproof room. 37
Various conditions that are recommended for BERA examination include: newborns to anticipate speech/language development disorders. If a child has a speech disorder or is slow to speak, one of the reasons may be because the child is unable to receive sound stimulation due to a disorder in the ear. 37 BERA can also be used to determine the source of hearing loss whether in the cochlea or retro cochlea, evaluate the brainstem, and determine whether hearing loss is caused by psychological or physical factors. This examination is relatively safe, painless, and has no side effects, so it can also be used for medical check-up screening. 37 Although BERA provides information on hearing function and sensitivity, it is not a substitute for formal hearing evaluation, and the results obtained must be able to be linked to the results of commonly used audiometry if available. 36,37
Mechanism inspection BERA is with give stimulation sound through The headphones that have been set at the control level will travel through the cochlea → cochlear nucleus → superior olivary nucleus → lateral lemniscus → inferior colicle → auditory cortex in the temporal lobe of the brain. The responses given will be received by the electrodes. Which affixed on skin And forwarded to computer so that the result can viewed on a computer screen
Auditory Steady State Response (ASSR)
Auditory Steady State Response or ASSR is an objective test to measure the hearing ability of children who are not yet able to undergo subjective test procedures. like play audiometry or audiometry pure tone. ASSR is also a test objective used for the evaluation of hearing ability in children for traditional audiometric testing.36,37
As with ABR, ASSR can also be used to estimate hearing thresholds. for they Which No can participate in steps Which traditional. Therefore, the main benefits for ASSR include: in infants for diagnostic follow-up assessment, infants in the neonatal intensive care unit (NICU), unresponsive and/or comatose patients, etc. 36
Basically, the examination method in the ASSR test is the same as the examination in BERA. What distinguishes it is the frequency examined and the description of the test results. The results of the BERA test are in the form of waves while the results of the ASSR test are in the form of an audiogram. 36
Management
Syndrome rubella congenital No have Treatment specific, only supportive. Part big baby SRK need maintenance multidisciplinary and maybe need intervention medical, surgery, development, and rehabilitation.
Joint Committee on Infant Hearing (JCIH) 2000 established disturbance hearing loss in children should be detectable at 3 months of age and appropriate interventions are initiated at the age of 6 months. Intervention said with amplification through installation hearing aids (ABM), cochlear implantation, and special education (speech therapy, SLB-B) as rehabilitation efforts, so that it is hoped that children can achieve optimal speaking and language skills. 38
Tool Help Hear
Tool help hear is a tool acoustic electricity Which can used by human with dysfunction hearing on the ear. Usually this tool can be installed on the inside of the ear or on the area around the ear. The hearing aid is made to strengthen the stimulation of the damaged sensory cells of the inner ear to stimuli. voice And sound sound from outside. Aids hear that is A electronic device that uses batteries where in use there is a microphone that changes the sound wave from voice the become energy electricity Which Then accepted amplifier that can increase the volume of sound and send it to the speaker located in the inner ear. 39Age at the time of amplification has a major influence on speech perception and production abilities. words, And language. Factors that influence use hearing aids in children include the mother's level of knowledge, chronological age, and degree of deafness. Hearing aids in children child Which most often chosen is the tool that placed in behind ear. Type of tool this is recommended by American Academy of Audiology for child Because own risk the smallest For swallowed by children compared with hearing aids in in ear. For Children with bilateral deafness are recommended to use bilateral hearing aids. The advantage of this device is that it can improve binaural hearing including auditory localization and nasal speech understanding. During the first two years of hearing aid use, The Pediatric Working Group recommends that audiology consultations should be carried out periodically 22 every 3 months to monitor audiological status and hearing aid fit because of rapid ear canal growth during this period. The consultation period can be accelerated if there are problems or risks of progressive deafness. 40

Picture 7. Tool help hear 39
Implant Cochlea
Implant cochlea is tool prosthetic Which designed And implanted on cochlea to convert mechanical sound energy into electrical signals that directly stimulate the auditory nerve in people with severe-profound hearing loss. Cochlear implants replace the function of damaged cochlear hair cell transducers. This device has become the treatment of choice standard in rehabilitation sufferer Which No helped with tool help conventional hearing . 39
Cochlear implants directly stimulate the spiral ganglion cells which are the first receptive neurons in the auditory pathway. Cochlear implants usually have low complications, although severe complications can occur such as facial nerve trauma (0.39%), fluid fistula cerebrospinal or perilymphatic (0.25%), and meningitis (0.11%). The use of cochlear implants has been approved by the Food and Drug Administration (FDA) in children over 12 months of age. However, some literature suggests continued auditory rehabilitation and language development after cochlear implant placement. Collerti et al reported better receptive language development (20-100%) after 9 years of cochlear implant placement. Cochlear implants have been reported to be clinically effective. 40

Picture 8. Implants cochlea
Initially, cochlear implants were only recommended for children with severe sensorineural hearing loss who did not benefit from conventional hearing aids; However guidelines This has expanded For consider implant cochlear for children with less severe hearing loss. 40 For children with hearing loss sensorineural bilateral, AIDS hear bilateral usually recommended For children with remainder hearing Which Enough. For children with disturbance severe to profound hearing loss, hearing aids may not be sufficient rehabilitation of hearing loss and cochlear implant technology should be considered. The advent of cochlear implants has enabled many children with bilateral severe to profound hearing loss to achieve age-appropriate speech. 41
Provision tool help hear And implant cochlea since early has proven help many children reach ability talk And Language Which approach normal, Which measured with growth curve . 41.42
There are various methods to evaluate a child's development after a cochlear implant. One of the internationally recognized methods for assessing the development of auditory perception is is with use method Category Performance Auditory (STAMP). Method CAP is a receptive scale assessment of auditory stimulation that can be applied to all child without look at age, before And after implantation. Method STAMP moment This is being developed into the CAP-II with more assessment scores. Several studies have shown that age at implantation affects hearing and language. Earlier implantation results in better development. Many children who are implanted implant before age 2 year own ability talk And Language Which The same with children of the same age who do not have hearing impairments 43
Prevention And Screening
Prevention is the key The main thing is to control incidents SRK, namely through the program Immunization. Centers for Disease Control (CDC) recommend dose first vaccine Measles, Mumps and Rubella (MMR) at 12-15 months of age, second dose at 4-6 years of age. The first dose is to reduce CRS complications and the second dose is to prevent transmission. virus rubella. Age mature Which Not yet Once get vaccine can done one dose of MMR vaccine. Women of childbearing age can be given the vaccine one month before pregnancy. 32
Prevention is carried out by examining IgM and IgG antibodies ELISA against rubella on all woman Which plan pregnancy and pregnant women who have symptoms infection rubella. Level IgG ≥15 IU/mL generally considered can protect the fetus to rubella. If No own immunity, avoid exposure rubella, and keep cleanliness self. Vaccine rubella No can given to woman pregnant Because can pass placenta. Woman age fertile Which Possible pregnant, need received a single dose of vaccination. Advisory The Committee on Immunization Practices (ACIP) recommends so that pregnancy avoided during 28 day after every dose live vaccine. Immunization passive does not prevent infection fetus if the mother is infected. Vaccination since childhood or before pregnancy. For protection against Rubella virus attacks, a vaccine is available in the form of a combination vaccine which is also used to prevent measles and mumps infections, known as as the MMR vaccine (Mumps, Measles, Rubella). Rubella vaccine is given at age 15 month. After That must get test on age 4-6 year. When Not yet get a repeat at the age of 4-6 years, must still be given the age of 11-12 years, even until adolescence. 10
Hearing loss according to The Joint Committee on Infant Hearing (JCIH) is diagnosed and intervened before the age of 6 months. Early detection in all newborns should be done at the age of 1 month, diagnosis at the age of 3 months, and intervention at the age of 6 months. Babies born with sensorineural hearing loss and hearing loss before 4 years old will forget all memories And speech. Children who are detected and intervened before the age of 6 months had significant differences in language abilities compared to children who were detected and intervened after the age of 6 months 44
The Joint Committee on Infant Hearing has now recommended screening to detect various disturbance hearing on neonate. Screening This done on babies under the age of 1 month, then back evaluated at the age of 3 months And 6 months. Currently, 97% of infants in the United States have been screened for hearing. OAE and ABR are techniques commonly used in hearing loss screening. 40
REFERENCE
IDAI, 2016. Handryastuti, S, Congenital Rubella Syndrome , Available from http://www.idai.or.id/artikel/klinik/keluhan-anak/sindrom-rubela- kongenital
Ezike E, Steele RW, 2013. Pediatric Rubella. Available from URL: http://emedicine.medscape.com/article/968523.
Banatvala, J.E., and DWG Brown.2014. Seminar Rubella.The Lancet. Vol. 363: 1127- 1137.
Dammeyer, Jesper. 2010. Congenital Rubella Syndrome and Manifestations. International Journal of Pediatrics Otorhinolaryngology. Vol 74 : 1067-1070
Smith, JH Richard, James F. Bale, Karl R. White. 2015. Seminar on Sensorineural Hearing Loss in Children. The Lancet. Vol 365: 879-90.
Karimi-Boroujeni M, Zahedi-Amiri A, Coombs KM. Embryonic origins of virally induced hearing loss: a review of molecular etiology. Viruses 2021; 13(1):71. https://doi.org/10.3390/v13010071
Ministry of Health. Status measles and rubella At the moment in Indonesia [Internet]. [cited 2018 Nov 9]. Availablefrom: http://www.searo.who.int/indonesia/topics/immunization/mr_measles_stat us.pdf?ua=1
Djelantik BD. Progressive autosomal dominant hearing loss due to a genetic defect on chromosome 1 in families from West Java. An audiologic and genetic study (PhD thesis). Antwerp: Antwerp University, Belgium; 2009.
Dewi YA, Agustian RA. Characteristics of congenital sensorineural hearing loss in children Which detected with brain stem evoked response audiometry. MKB. 2011;43:77-82.
Tian C, Ali SA and Weitkamp JH, 2010. Congenital Infections, Part I: Cytomegalovirus, Rubella and Herpes simplex. Neoviews 11(8):e436-45.
Choo, D, I, Richter, G, T. 2009. Development of the ear, In: Snow, JB, Wackyym, PA (eds) Ballenger's otorhinolaryngology head and neck surgery. Connecticut: BC Decker Inc., p.17-26.
Wareing, M, J, Lalwani, A, K, Jackler, R, K. 2006. Development of the ears, In: Bailey, B,J, Jonas, J,T, Newlands, S,D, (eds) Head & neck surgery otolaryngology. Philadelphia: Lippincott Williams & Wilkins, p. 1869-80
Wright, A. 2007. Anatomy and ultrastructure of the human ear, In: Kerr, AG (ed) Scott- Brown's otolaryngology. Vol.1, London: Butterworth- Heinemann. h. 1/1/1-10
Dhingra, P,L. 2010. Disease of ears, nose, and throat, 4th ed. New Delhi: Elsevier, h. 3- 15.
Wikipedia. 2013. Organ of Corti, Available from: http://en.wikipedia.org/wiki/Organ_of_Corti. [accessed 30 December 2018]
Good luck, R. 2009. Anatomy of the auditory and vestibular system, In: Snow, JB, Wackyyym,
PA (eds) Ballenger's otorhinolaryngology head and neck surgery. Connecticut: BC Decker Inc., p. 1-15.
Mills, J, H, Khariwala, S, S, Weber, P, C. 2006. Anatomy and physiology of hearing, In: bailey, B,J, Johnson, J,T, Newlands, S,D, (eds) Head and neck surgery – otolaryngology. Texas: Lippincott Williams &wilkins, p. 900- 1887
Laura, T,L, Abraham, K,L. 2012. Cell Biology, Histology and cell biology. 3rd edition. Elsevier. Oxford.
Ingber, D, E. 2006. Cellular mechanotransduction: putting all the pieces together again, FASEB J. 20, p.811-27
Kadek, Darmadi S, 2007. Symptoms of Congenital Rubella (Congenital) based on Serological Examination and RNA Virus. Indonesian Journal of Clinical Pathology and Medical Laboratory :13(2):63-71.
Victor, F, Rosa Andrea, P, Silvia, C, T. 2012. Genetics of congenital deafness next document med clin (Barc), Elsevier. 139, pp. 446-51.
WHO. Global and regional immunization profile [Internet]. 2018 [cited 2018 Nov 9]. Availablefrom: http://www.who.int/immunization/monitoring_surveillance/data/gs_glopr ofile.pdf
Ministry of Health. Instruction technical campaign immunization measles rubella (MR). 2017
McLean H, Redd S, Abernathy E, Icenogle J, Wallace G, 2012. Chapter 15: Congenital Rubella Syndrome. In: VPD Surveillance Manual. 5th Ed
Giambi C, Philia A, Rotation MC, Manso MD, Declich S, Nacca1 G, Rizzuto E, Bella A, 2014. Congenital rubella still a public health problem in Italy: analysis of national surveillance data from 2005 to 2013. Surveillance and Outbreak Reports.
Nguyen TV, Pham VH, Abe K, 2015. Pathogenesis of congenital rubella virus infection in human fetuses: viral infection in the ciliary body could play an 44 important role in cataractogenesis. EbioMedicine, 2: 59–63.
Lin C, Shih S, Tsai P, Liang A, 2015. Is birth cohort 1985/9-1990/8 a susceptibility window for congenital rubella syndrome in Taiwan?. Taiwanese journal of Obstetrics & Gynecology.
Quintana EM, Solórzano CC, Torner N, Gonzalez FR, 2015. Congenital rubella syndrome: a matter of concern. Pan American Journal of Public Health, 37 (3): 179- 186.
Soetjipto, D. 2007. Congenital Deafness. National committee for the prevention of hearing disorders and deafness, Available from: http://www.ketulian.com/v1/web/index.php?to=article&id=14. [accessed 30 November 2018]
Lee, JY, Bowden DS (2000) Rubella virus replication and links to teratogenicity. Clinical Microbiology Reviews 13 (4):571-587.
Donley DK (2013) TORCH infection in the newborn. Seminars in Neurology 13 (1): 106-115
HTA Indonesia. 2010. Book Guide Treatment Baby New Born in House Sick. 39(9),h. 538- 42
McPherson RA, Pincus MR. Henry's clinical diagnosis and management by laboratory methods. 23rd ed. St. Louis, Missouri: Elsevier; 2017.
Hall III, J, W, Antonelli, P, J. 2006. Assessment of peripheral and central auditory function, In: Bailey et al, BJ, Jonas, JT, newlands, SD (eds) Head &Neck surgery otolaryngology. Philadelphia: Lippincott Williams & Wilkins, p. 1927-42.
James W, Patrick J, Antonelli. Assessment of Peripheral and Central Auditory Function. In: Bailey BJ, editor. Head and Neck Surgery Otolaryngology. Edition fourth. Philadelphia: Lippincott Ravens. 2016. p.1928-42.
Probst R, Grever G, Iro H. Detection and Investigation of Pediatric Hearing Disorders. In: Probst R, Grever G, Iro H, editors. Basic Otorhinolaryngology : A Step by Step Learning Guide. Second edition. New York: Georg Thieme Verlag. 2006. p.198-201.
Johnson KC. Audiologic Assessment of Children with Suspected Hearing Loss. Otolaryngol Clin N Am. 2012; 35: 711-32.
Dewi YA, Agustian RA. Characteristics of congenital sensorineural hearing loss in children detected by brainstem evoked response audiometry. MKB. 2011 ;43:77-
82.
Gurtler, N. 2008. Hereditary hearing impairment, In: Lalwani, AK, Ed. Current Diagnosis & Treatment in Otolaryngology Head and Neck surgery. Second edition. USA: The McGraw Hill, 697-704
Leger J. Congenital hypothyroidism: a clinical update of long-term outcome in young adults. European society of endocrinology. 2015; 172(2):67-77.
Sarant J, Harris D, Bennet L, Bant S. Implants bilateral cochlea versus unilateral in children: a study of oral language outcomes. Ear Hear. 2014;35(4):396-409. doi:10.1097/AUD. 022
Leigh J, Dettman S, Dowell R, Sarant J. An evidence-based approach to making cochlear implant recommendations for infants with residual hearing. Ear Hear. 2011;32(3):313-322. doi:10. 1097/AUD.0b013e3182008b1c
Arief W, Zizlavsky S, Priyono H, Wahyuni LK, Medise BE, Prihartono J. Description of CAP-II auditory perception in bilateral prelingual deaf children 6-12 months after cochlear implantation. ORLI 2018;48(1):1-10. https ://doi.org/10.32637/ orli.v48i1
Ekorini HM. Report on the cochlear implant program at Dr. Soetomo Hospital, Surabaya. ORLI 2016; 46(1):8-15. https://doi.org/ 10.32637/orli.v46i1.142
Comments