DIPHTHERIC TONSILLITIS
I Made Nudi Arthana
Diphtheria Tonsillitis is one of the causes primary tonsillitis and pharyngitis in individuals Which No immunized And own system immunity body Which weak, which can cause significant death and morbidity if left untreated.
LITERATURE REVIEW
Definition
Diphtheria is Wrong One disease Which very infectious, can prevented by immunization, And due to by bacteria grams positive Corynebacterium diphtheriae strain toxin. Disease This marked with existence inflammation at the site of infection, especially on the mucous membranes of the pharynx, larynx, tonsils, nose and also on skin. Man is the only one reservoir Corynebacterium diphtheriae . Transmission happen in a way droplet (splash) saliva) from cough, sneeze, vomiting, through tool Eat, or contact direct from lesi in skin. Sign And symptom in the form of upper acute respiratory tract infection (URTI), sore throat, pain when swallowing, fever No tall (not enough from 38.5 0 C), And found the presence of a white/greyish/blackish pseudomembrane in tonsils, pharynx, or larynx that are not easy off, as well as bloody If lifted. As many as 94 % case Diphtheria affects the tonsils and pharynx. In more severe cases it can be characterized by difficulty swallow, congested breath, stridor And swelling neck Which looks like neck cow ( bullneck ). Death usually happen Because road obstruction breath, damage muscle heart, as well as abnormality arrangement nerve center And kidneys. 10 The most common locations of diphtheria infection are the tonsils and pharynx. Infection at these locations
This is usually associated with systemic absorption of large amounts of toxin. Initial symptoms include malaise, sore throat, anorexia, and mild fever (<38.5 o C). Within 2-3 days, a bluish-white membrane forms and expands to varying sizes. The pseudomembrane is greenish-gray or black if bleeding has occurred. The mucosa around the pseudomembrane appears erythematous. 9 Extensive pseudomembrane can result in airway obstruction. Patients with disease heavy can experience edema in area submandibular And neck part front throughout area gland gertah clear neck, so that show a picture “ bullneck ”. If the toxin that absorbed by the body Enough Lots, patient very weak, pale, tachycardic, stuporous, coma, and even death within 6-10 days. 9Definition case operational surveillance diphtheria: 10
Diphtheria suspects are people with symptoms of pharyngitis, tonsillitis, laryngitis, tracheitis, or a combination of these accompanied by a low fever and the presence of a grayish white pseudomembrane that is difficult to remove and bleeds easily if removed or manipulated.
Probable Diphtheria is person with suspect Diphtheria added with one of the following symptoms:
Once contact with case (<2 weeks).
Immunization No complete, including booster Which Not yet done.
Is at in area endemic Diphtheria.
Stridor, Bullneck .
Bleeding submucosa or petechiae on the skin.
Fail heart, fail kidney I.
Myocarditis.
Die.
Laboratory confirmed cases are suspected cases of diphtheria with positive culture results for toxigenic strain Corynebacterium diptheriae or positive PCR ( Polymerase Chain Reaction ) for Corynebacterium diptheriae which has been confirmed by the Electron test.
Epidemiologically linked confirmed cases are cases that meet the criteria for suspected diphtheria and have an epidemiological link with laboratory confirmed cases.
Clinically compatible cases are cases that meet the criteria for suspected diphtheria but do not have an epidemiological relationship with laboratory-confirmed cases (point 1 above) or epidemiologically linked confirmed cases (point 2 above).
Contact cases are people in the same house, playmates, schoolmates, including teachers and close contacts of work colleagues with the case.
A carrier case is a person who does not show clinical symptoms, but laboratory test results show positive for Corynebacterium diphtheriae.
Epidemiology
Since the vaccine was implemented, the incidence of diphtheria has decreased significantly. fast. Before year 1920, US report around 200,000 case per years. However, this number has decreased drastically after the introduction of widespread immunization programs, with only about 1000 cases reported each year. Most cases are found in individuals of low socioeconomic status, stay in area Which congested resident, not enough immunization, own travel history from area endemic, And own condition comorbidity. These figures remain higher in some global regions, particularly Southeast Asia and Africa. About number death in US, the numbers has decrease from 100 to 200 cases to 0.001 per 100,000 population since the introduction of vaccination. Reports from WHO indicate that diphtheria epidemics continue to pose a health risk in developing countries. India has a higher incidence of diphtheria, mainly due to challenges in implementing widespread vaccination efforts. The majority of the global diphtheria burden is concentrated in India. 11,12 Diphtheria does not show any racial or sexual preference. Although diphtheria is generally known as a childhood disease, affecting primarily those under 12 years of age, individuals around 40 years of age and those with comorbid conditions are also susceptible to infection. As immunity to the bacteria naturally wanes, the risk of infection increases for individuals who are not currently immunized and have not received booster doses. 13
Diphtheria cases in Indonesia experienced a spike in the period 2015-2021. From 2015 to 2018, the number of diphtheria cases increased. case that is 529 case on year 2015, 591 case in year 2016, 954 cases in 2017, 1,386 cases in 2018. Then in 2019 to 2021, diphtheria cases in Indonesia decreased, namely 529 cases in 2019, 259 cases in 2020, and 235 cases in 2021 (Ministry of Health, 2021). 14 In year 2022, case diphtheria spread almost in all over province in Indonesia except for 6 provinces, namely East Nusa Tenggara, Maluku, South Papua, Central Papua, Papua Mountains, and Southwest Papua. The number of diphtheria cases in 2023 was 949 cases. This figure shows an increase of almost two times fold from case diphtheria Which happen on year 2022, that is as much as 541 cases. Over the past 2 years, the number of deaths due to diphtheria has increased significantly. In 2022, the number of deaths was 46 cases, becoming 68 cases in 2023. Of the 38 provinces with diphtheria cases, 16 provinces found cases of death due to diphtheria. The highest number of deaths occurred in West Java Province with 21 cases, followed by North Sumatra with 10 cases and East Java with 9 cases. In 2023, the Case Fatality Rate (CFR) for diphtheria cases in Indonesia was 7.2%, a decrease compared to 2022, which was 9%. From 16 province with case death diphtheria, number CFR most tall happen in Southeast Sulawesi Province at 37.5%, followed by Central Sulawesi at 33.3% and North Sumatra at 30.3%. 15 In a case investigation in Kediri, 5 different suspected cases were found in Kediri Regency in 2022 with clinical symptoms Which experienced fifth patient that is fever, Sick throat, swelling in the neck, shortness of breath, and pseudomembrane. 16
Etiology And Risk Factors
Corynebacterium diptheriae was first described in 1884 by Friedrich Löffler, who also showed that this bacterium was the causative agent of diphtheria. 22 Corynebacterium diphtheriae , a gram-positive, aerobic, non-encapsulated, non-motile bacillus, is the bacterium that causes diphtheria. The main risk factor for contracting the disease is lack of immunization. Although individuals can carry the bacteria without symptoms, it often affects the respiratory and integumentary systems. Humans are the only hosts for the organism, which resides in the upper respiratory tract, and transmission bacteria happen through droplet in air. C. diphtheria is basil gram-positive, non-spore-forming bacterium characterized by its non-motile and non-encapsulated nature. Its club-shaped appearance forms a palisade or arrangement shaped V or L. Besides C. diphtheria , Corynebacterium ulcerans can cause cutaneous diphtheria and, rarely, contribute to cases of respiratory diphtheria. 17 The pathogenic impact of exotoxins extends from localized to systemic manifestations of the disease. Viral bacteriophages carry the genetic code for exotoxins, which facilitates their transmission between bacteria. Three different strains of C diphtheriae gravis, intermedius, and mitis have been isolated, and all three are capable of produce toxin. There is also the type C.diphtheriae belfanti which is one of the strains that does not produce toxins. 17
Pathogenesis diphtheria involving various factor etiology, including incomplete or no immunization, decreased immunity over time, make person carry on age Which No get vaccination booster more susceptible to infection, low herd immunity, travel to endemic areas, travel to areas experiencing a current epidemic, socioeconomic status, large-scale population movements, overcrowded conditions, such as military barracks, prisons, and homeless shelters, pets. 18 A systematic review showed low immunization coverage, difficulty in accessing immunization services, and low income levels. is factor Which trigger the emergence incident outside normal in developing countries. Strengthening surveillance and health service systems is essential to address diphtheria outbreaks. 19
A study by Nassar et al. found that vaccination, not sharing a bedroom, with at least two person, And isolation case diphtheria For prevent contact with uninfected people are the most important steps to protect the community from diphtheria. It is recommended to increase public awareness about vaccination, transmission, And steps prevention. In total, 76 confirmed cases and 152 controls were enrolled in this study. Multivariate analysis found a significant association between diphtheria infection and sharing room Sleep with at least two person (aOR 2.8, 95% CI 1.2–6.6), not vaccinated (aOR 2.6, 95% CI 1.2–6.0) And contact with case diphtheria (aOR 10.6, 95% CI 2.6–43.6). 20 Other studies confirm the association between increasing diphtheria cases, immunization coverage, and ongoing conflict. A total of
1,294 probable cases of diphtheria were reported from 177 areas with a high mortality rate. case overall as big as 5.6%. Around 65% patient is children in under the age of 15 years, and 46% of cases had never been vaccinated against diphtheria. The risk plague increase 11 time fold If area the experience conflict which is being in progress p < 0.05. If happen conflict (Good Which Already passed or ongoing), the risk of an outbreak decreases by 0.98 if immunization coverage is high p > 0.05. 21
Pathophysiology
C. diphtheriae almost exclusively found in humans, although other animals other, including cat, dog, horse, And animal Pet other, may also be potential carriers of this organism. Infected individuals and asymptomatic carriers can act as a source of transmission of C. diphtheriae through droplet breathing, secretion nose, and rarely through contact contaminated objects. Diphtheria on channel breathing on spread from person to people through droplet breathing. Besides That, secretion other And material contaminated can become source infection, especially in case diphtheria skin, in where wound or insect bites are common entry points. 23
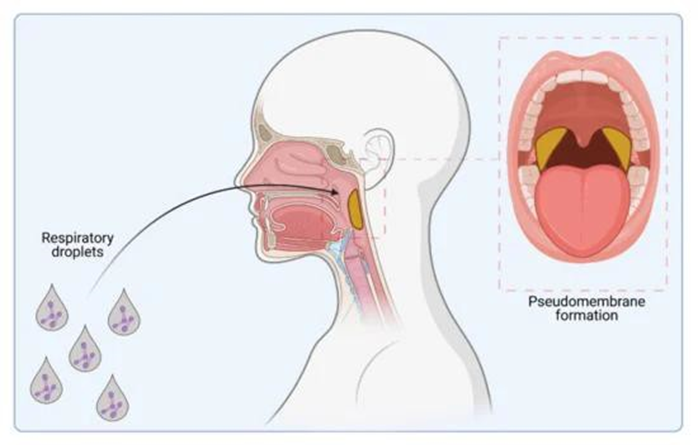
Picture 1. Infection C. diphtheriae . Track infection through droplet breathing and pseudomembrane formation (shown in yellow) is caused by colonization of the upper respiratory tract. 23
Adhesion on C. diphtheriae mediated primarily by pili (or fimbriae) which attached in a way covalent on wall cell bacteria And contribute on colonization in host. Pathogen This contain three group gene pill Which encodes nine pilus proteins, SpaA–SpaI, known as the mediated pilus proteins sorting (or twist). Every protein Spa contain motive LPXTG, the split by enzyme sorting And own role important in colonization, virulence, and infection by Gram-positive pathogens. Isogenic mutants of toxigenic C. diphtheriae strains , Which No own gene Which coding protein pill type SpaA (SpaA, SpaB, And SpaC) (ΔspaABC), show murder Caenorhabditis elegans , thus demonstrating the importance of pili in pathogenicity. The minor pilins SpaB and SpaC act as specific adhesins that facilitate bacterial attachment this to the cell pharynx host, which is very decreases when These proteins lack pili. The host cell receptors targeted by SpaB and SpaC have not been identified, nor have the specific effects of SpaH-type pilus proteins (SpaH, SpaI and SpaG) on clinical outcome. Lipoarabinomannan-like lipoglycans and the cell surface proteins DIP1281 and DIP1621 have also been identified as adhesive factors in C. diphtheriae . Low iron availability has been shown to alter cell adhesion and the expression of surface carbohydrate moieties, which may influence the progression of C. diphtheriae infection . 24
Production toxin or Diphtheria Toxin (DT) is factor virulence The main genes involved in the pathogenesis of this disease. The genes responsible for toxin synthesis are encoded by corynebacteriophage , and when integrated into the bacterial genome, have the potential to transform non-toxigenic strains into toxigenic strains. Which virulent. Gene bacteria This consists of from chain polypeptide single consisting of 535 amino acids. Further analysis of the toxin by X-ray crystallography along with genetic and biochemical analysis revealed that it consists of three functional domains, namely a catalytic domain with N-terminal ADP ribosyltransferase activity , a transmembrane domain assisting in the delivery of the catalytic domain across the cell membrane, and a cell receptor-binding domain. After binding of the diphtheria exotoxin to the host cell receptor, it undergoes receptor-mediated endocytosis. The toxin then undergoes endocytosis, where it is acidified. The transmembrane domain is then inserted into the membrane, allowing delivery domain catalytic to the cytosol. Domain catalytic catalyze
ribosylation of NAD+-dependent elongation factor 2 and thereby inhibits protein synthesis. Although bacteria acquire the toxin-producing gene from bacteriophages, its signaling regulation is controlled by the bacteria. The diphtheria toxin repressor gene (DtxR) is present on the bacterial chromosome, and toxin production depends on expression toxin And metabolism substance iron bacteria. DtxR is repressor gene activated by metals and responsible for the regulation of iron uptake and the expression of hem-oxygenase and diphtheria toxin. Siderophore is responsible for transporting iron into the bacterial cell. After iron binds to the Siderophore , a conformational change occurs in its structure which in turn allows the repressor to bind to the toxin operator site. Regulation of the toxin by DtxR is dependent on the availability of iron. DtxR is inhibited by a decrease in iron concentration and therefore results in an increase in the amount of toxin formation. 24
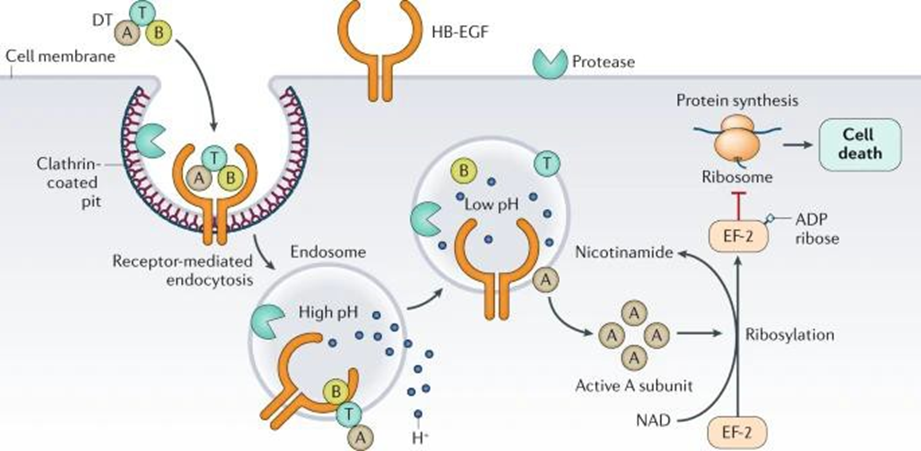
Picture 2. Mechanism Toxin Diphtheria. 24
Absorption and spread of diphtheria toxin through blood circulation from the respiratory tract can cause the most systemic effects often manifested as damage on myocardium And nerve edge, Which cause complications such as myocarditis, peripheral neuropathy, and polyneuropathy. Diphtheria Toxin or DT can be fatal to humans at doses below 0.1 μg/kg body weight. Precursor HB-EGF act as receptor For DT on membrane plasma human cells, especially on neuron cerebral And myocyte heart. Cytotoxicity Which induced DT varies, Because involving division DNA And cytolysis (by inhibiting eukaryotic translation elongation factor 2 (EF-2) via ADP-ribosylation and actin filament depolymerization. DT-induced actin filament degradation is important because the toxin is known to cause the severe, often fatal, cardiomyopathy associated with diphtheria. 24
Diagnosis
Anamnesis
Initial symptoms include malaise, sore throat, anorexia, and mild fever. (< 38.5°C). In 2-3 day, formed bluish-white membrane And expanding and of varying size. A history of travel from an endemic area without a record of vaccination is often indicative. In such cases, the health care practitioner should be alert to the characteristic features of the disease, particularly the presence of a thick, gray, adherent pseudomembrane covering the tonsils and throat. Respiratory tract involvement is common, beginning with mild erythema that progresses to a coalescing pseudomembrane. 17
Pseudomembrane is greenish-gray or black if bleeding has occurred. The mucosa around the pseudomembrane appears erythematous. Extensive pseudomembrane can result in airway obstruction. Patients with severe disease may experience edema in the submandibular area and anterior neck along the lymphadenopathy area, thus showing a “ bullneck ” appearance. If the toxin absorbed by the body is large enough, the patient is very weak, pale, tachycardic, stuporous, coma, and even dies within 6-10 days. The main cause of death is airway obstruction or suffocation, mainly due to aspiration of pseudomembrane. 9,25 In a study, clinically, all patients had fever and severe sore throat. On clinical examination, 31 cases (93.7%) had pseudomembrane over the tonsils, 26 (78.1%) had bullneck (multiple cervical lymph node enlargement), and 28 (84.8%) had difficulty breathing when they came to the hospital. 26
Cardiac manifestations may include myocarditis, conduction defects leading to heart block. total, and cases fail heavy heart. Matter This Also can cause demyelination nerve And neuropathy Which as a result, start from mild weakness to complete paralysis. Several presentations resembling Guillain Barre syndrome have also been reported in the past. It is also known that diphtheria toxin can cause diphtheria polyneuropathy through inhibition of myelin proteolipid and essential protein synthesis, which initially presents as palatal paralysis, then progresses to distal polyneuropathy, diaphragmatic paralysis, and finally death. Cutaneous manifestations can cause cutaneous diphtheria. Cutaneous diphtheria appears as chronic ulcers that do not heal healed in part body Which open, usually hand, legs, and feet. Clinically, cutaneous diphtheria is indistinguishable from ulcers caused by other organisms and often occurs in association with Staphylococcus and Streptococcus infections. 4
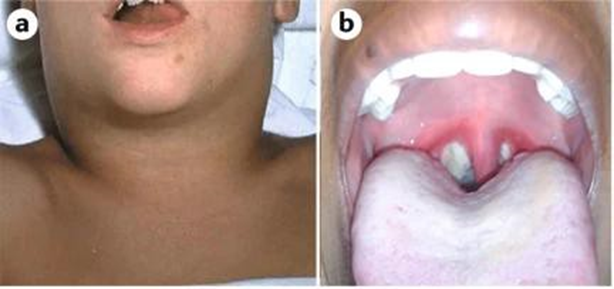

Figure 3. ( a) Characteristic “ bullneck ” caused by swollen glands sap clear. (b) Pseudomembran thick in the tonsils And pharynx posterior. Pseudomembrane is a layer of bacteria and debris from surrounding tissue necrosis due to diphtheria toxin. (c) Skin lesion caused by Corynebacterium diptheriae . 24
Physical examination
Patients usually have a low-grade fever but appear very lethargic, often with a swollen neck. Common symptoms include fever, tachycardia, halitosis, and anxiety. A thick, gray, leathery pseudomembrane covers the tonsils, oropharynx, soft palate, nasopharynx, and uvula. Scraping of the pseudomembrane causes bleeding into the underlying mucosa. Patients may hold their head erect because of the prominent neck. Occasionally, dysphonia may occur. Respiratory distress is manifested by stridor, wheezing, cyanosis, and retractions. 17
Table 2. Classification tonsillitis membranous 3.26
Classification | Tonsillitis Diphtheria | Tonsillitis Septic | Angina PlautVincent (Membranous Ulcerous Stomatitis ) |
Etiology | Corynebacterium Diphtheriae | Streptococcus hemolyticus found in cow's milk | Spirochaeta or triponema in patients with poor oral hygiene and vitamin C deficiency |
Physical examination | Tonsil swollen covered spots dirty white, gray and thick which expands over time and unites to form a pseudo membrane. This membrane can extend to the soft palate, uvula, nasopharynx, larynx, trachea, and bronchi which can block the airway. This membrane adheres tightly to its base when lifted. will easy to bleed. Swelling on the lymph glands that resemble a cow's neck " Bull Neck" | Swollen tonsilsand redness, sometimes there is pus/pus on tonsil | Oral and pharyngeal mucosa is hyperemic, looks grayish white membrane over the tonsils down to the gums and alveolar process and swelling of the submandibular glands |
Cardiac involvement occurs after 1 to 2 weeks of illness after resolution of the tonsil/pharyngeal phase. Cardiac involvement may manifest as myocarditis Which can appear in a way I with fail heart congestive and collapse circulation. Patient can own symptom like dyspnea progressive, spatial dilation heart, voice heart reduce, And weakness. Change wave ST- T, atrioventricular block, and various dysrhythmias may be seen.27 Neurological involvement depends on level infection tonsil And pharynx. Deficit covering nerve deficit cranial, neuropathy sensory peripheral Stocking And gloves, as well as neuritis peripheral. 17

Picture 4. Pseudomembran thick colored gray typical formed in tonsil and throat, Which potential cause blockage respiratory tract . 17
Supporting investigation
Culture Throat
Swabs are taken from pseudomembranes or lesions visible at the mucosal pillar border. tonsil And membrane Which formed For culture use identify C. diphtheriae . Throat swabs are cultured on specific media to isolate the bacteria. If allows, must wipe taken from under the pseudomembrane or a piece of membrane must be removed. A single swab from each nose and throat Also must taken in case diphtheria skin For to rule out the possibility of respiratory transmission of toxigenic strains. 17,28
Commonly used media include Löeffler or Tindale media, plates telluride, And so that blood. Characteristics special from media This indicates the presence of organisms: 17.24
Media Tindale : C. diphtheriae forms distinctive black colonies with light halos
Media Loffler : Details metachromatic observed with existence C. diphtheriae .
Preparation telluride: color gray-black typical tellurium shows the presence of organisms
Dacron, Viscose or flocked applicator swabs should be used to collect samples from each suspected case and placed in routine semi-solid transport media, such as Amies, immediately after collection and shipped. to laboratory microbiology House Sick For culture. Receptacle wipe should be appropriately labeled with a unique identifier, the source of the specimen, and the date of collection. If antibiotics have been started, specimens for culture should still be collected if within 24 hours of the first dose. Beyond this point, if appropriately treated, cultures are likely to be negative. Occasionally, there may be benefit in collecting swabs beyond this time point; for example, cutaneous diphtheria confirmed without respiratory examination. The physician should notify the local laboratory that diphtheria is suspected (or from a confirmed case, as appropriate). 17
Inspection Diphtheria Toxin
Since 1888, when Pierre Emile Roux and Alexandre Yersin isolated diphtheria toxin (DT) and showed that systemic disease manifestations relate with existence toxin, Lots study about DT detection has done. Detection toxin is test Which most important in microbiological diagnosis of diphtheria. Below, we present various methods for the detection of DT described in the scientific literature. 29,30
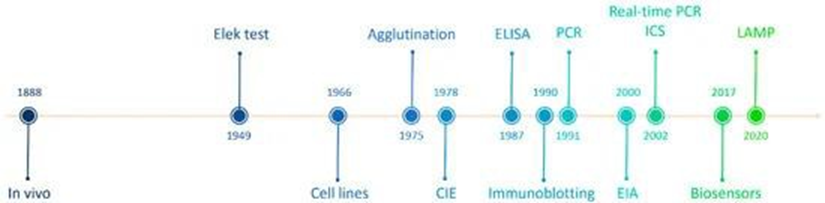
Picture 5. Detection toxin diphtheria in history. 30
Test Elek and Test Elek Modified
The Elek test is based on the principle of antigen-antibody precipitation. This test was first time described on year 1949, And since introduced, test This has replaced the traditional in vivo virulence test in guinea pigs, which was most common at that time. In this process, a positive control or toxigenic strain and a non-toxigenic strain or negative control along with a DAT-coated paper strip are placed in agar media. After 24 to 48 hours at 37 degrees C, the presence of a clear precipitation line at the junction where the toxin and antibody meet supports the diagnosis. Other enzyme-based tests such as catalase cystinase , pyrazinamidase nitrate , and urease nitrate urease can be used to diagnose potentially toxigenic species within 4 hours. 17
In studies by Melnikov et al., profit And loss from modifications to the previous Elek test were considered and the method was improved for the detection of pathogenic corynebacteria , including strains which is weakly toxigenic. The most critical point found on distance inoculum bacteria from disc antitoxin. Distance The optimum is 6 mm. The round shape of the bacterial inoculum and the 6 mm spacing appear to create ratio quantitative Which optimal between toxin And antitoxin. Besides that, form round plaque reduce possibility contamination cross between plaque adjacent. The specificity of the test can be increased by the use of pure antitoxin, which does not produce false-positive precipitin lines. When using antitoxin pure, the Elek test results can be evaluated not only after 24 hours, but even after 48 hours. After 48 hours of Elek test cultivation, the precipitin line became much more clear. If antitoxin Which No pure used in here, the result can only be determined after 24 hours, but cannot be read later due to the possibility of precipitation non-specific (Picture 6). Test Elek Also has simplified, Now No two but only One control positive used, and the amount of antitoxin has been reduced. 31
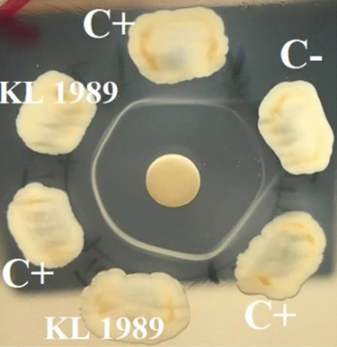
Picture 6. Test Elek Which optimized with isolate test KL 1989 after 48 hours of incubation at 37 °C with unpurified antitoxin. Non-specific precipitation lines were seen against the negative control. 31
Counterimmunoelectrophoresis
Counterimmunoelectrophoresis (CIE) was originally described by Bussard and Huer on year 1959 And used For detect antigen virus hepatitis (HBsAg) [43]. Almost 20 year Then, method This proposed For detecting DT in C. diphtheriae cultures , this method refers to the formation of a precipitation line in agar. This process is a modification of immunoelectrophoresis and takes place under the influence of an electric field. In CIE, antigen and antibody move in opposite directions, forming a precipitation at the point of their connection. In the results obtained, the presence of a precipitation line indicates the antigen corresponding to the antibody. In the CIE test, DT production can be detected within 16 to 24 hours. This test was developed using five toxigenic C. diphtheriae strains, one strain of C. diphtheriae non-toxicogenic, One C. hemolytic And three isolate diphtheria Which not determined, and the influence of culture media and culture conditions on the test results is shown. 30
Enzyme Linked Immunosorbent Assay (ELISA)
ELISA can be either a qualitative or quantitative method, with quantitative immunoassay methods based on mAbs being more easily standardized. Sandwich ELISA results include the results of other methods for DT detection, such as the Elek test or identification genetics gene tox, And characterized by sensitivity tall (around 99%) and specificity (100%). However, occasional false-positive results have also been documented. The detection limit of DT is less than 1 ng/mL. The use of ELISA to determine the level of toxin production by a strain can help in assessing the pathogenic potential of an isolate. This is especially important because epidemic diphtheria isolates cause a more severe form of infection in unvaccinated children as they produce greater amounts of toxin. Some writer has recommend that ELISA can useful as reference in vitro method for detecting isolates with questionable toxin production. 30 Research conducted by Simonova et al. showed that strain Corynebacterium with level DT Which low No detected by the Elek test and gave positive results in ELISA.32 Although the ELISA method is suitable For detect isolate diphtheria toxigenic in practice routine, This is a labor-intensive and time-consuming test. Another disadvantage is that there are no commercially available kits and all ELISA tests are based on internal method validation. 30
Enzymes Immunoassay (EIA)
Enzyme immunoassay (EIA) is a modification of the ELISA test for rapid diagnostics. EIA is also characterized by very high diagnostic sensitivity (LOD is 0.1 ng/mL). In a comparative study of 220 toxigenic Corynebacterium isolates , the results obtained by the EIA method were 100% consistent with those obtained by the Elek test. This method is quite accurate and specific for detecting toxigenicity. EIA provides results within 3 hours of colony picking compared to 24 hours for the modified Elek test. And 48 O'clock For test Elek conventional. More Far, interpretation EIA results are easier than for the Elek test. Isolates that show weak precipitation lines in the Elek test give a good visible color change. in EIA. To improve the detection of isolates with DT biological activity, standardization of inoculum density and incubation time in broth is essential, especially among isolates producing low levels of toxin. 30
Polymerase Chain Reaction (PCR)
nucleic acid amplification tests (NAATs) used for toxin detection were based on conventional polymerase chain reaction (PCR), in which product PCR Which colored with fluorescence separated on gel agarose, and explained on year 1990s. System PCR Which explained at first focused on the amplification of the A fragment of the toxin gene (toxA), which encodes the catalytic subunit of the toxin. In contrast, the later system, which is an extension of the previous system with additional primer sets, also amplifies the B fragment of the gene (toxB), which encodes the translocation and receptor-binding domains. The PCR by Hauser et al. targeted both the A and B fragments in a single amplicon (toxAB). The calculated LODs ranged from 50 to 1500 CFU/PCR mixture. The toxA amplification primer set was found to be more sensitive than the toxB primer set. Data from various studies have shown a 100% correlation between the results of these three conventional PCR systems and phenotypic methods, such as in vivo ADP-ribosylation activity and the Elek test. Faster and more sensitive detection of toxigenicity compared to with PCR conventional achieved with use PCR real-time, a method that monitors the amplification of target DNA during the process. This method involves amplification of toxA and toxB fragments and real-time detection using a hydrolysis probe (TaqMan). 30
Biosensor
Biosensors are a new technology that has been developed for diagnostic purposes. in a number of year final. Biosensor is probe analytical specific that consists of from part biological Which functioning as sensor And transducer which converts biological changes into signals that are proportional to the concentration of the agent being detected. 33 There are two main groups of biosensors, namely: (i) optical biosensors, Which often use resonance plasmon surface (SPR), colorimetry and fluorescence; And (ii) biosensor electrochemistry Which usually based on on impedance, amperometry and voltammetry. According to the literature, there are only a few biosensors developed to detect DT or DT gene. The function of the biosensor for DT detection is similar to the technology used in the ELISA test, while the biosensor for tox gene detection is based on the phenomenon of specific DNA strand hybridization. 34
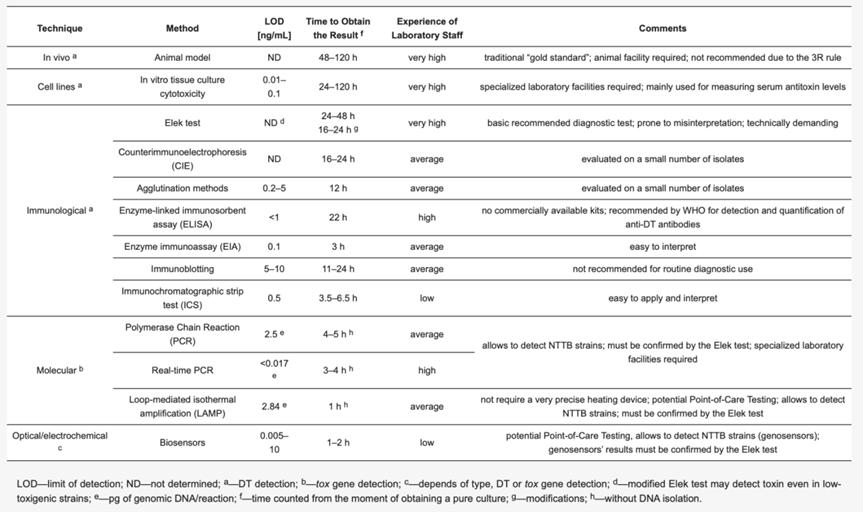
Picture 7. Method detection toxin diphtheria. 30
Radiology Examination
A chest X-ray may be performed if there are respiratory symptoms or concerns. about complications like pneumonia, X-ray chest can performed to assess lung involvement. This imaging test can reveal swelling of the soft tissue structures in and around the pharynx, epiglottis, and chest. An echocardiogram is performed in cases of suspected cardiac involvement, an echocardiogram can help assess the function and structure of the heart and may to reveal vegetation valve, although This is phenomenon rare. 17
Inspection Laboratory Other
Elevated leukocytes may indicate an inflammatory response. Troponin levels may be useful in assessing the extent of myocardial damage, to see if complications of myocarditis occur. 17
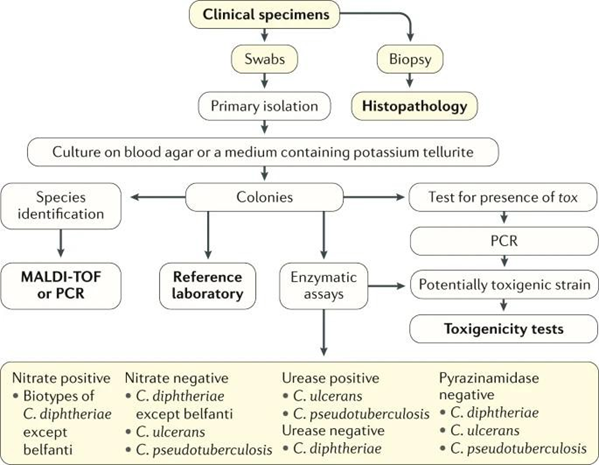
Picture 8. Algorithm Diagnosis. 24
TREATMENT
In cases of diphtheria, management begins with the administration of Anti-Diphtheria Serum (ADS) and antibiotics without the need for laboratory confirmation (culture, either swab/smear). throat). Sufferer diphtheria isolated until No infectious that is 48 hours after antibiotic administration. However, culture is still performed after antibiotic administration. Antibiotic administration aims to eradicate Corynebacterium diphtheriae stop production toxin, treat infection local, And prevent transmission of germs, not as a substitute for antitoxins which are the main therapy. Choice antibiotics For diphtheria is erythromycin, penicillin, azithromycin or clarithromycin. Erythromycin can given in a way injection or oral with dose 40- 5- mg/kgBW/day divided into 4 doses with a maximum dose of 2 grams per day for 14 day. Penicillin procaine G given every day in a way intramuscular or intravenously at a dose of 300,000 IU/day for body weight less than 10 kg and a dose of 600,000 IU/day for body weight more than 10 kg for 14 days. For the administration of ADS to patients, it is necessary to consult a Specialist Doctor (Pediatrician, ENT, Internal Medicine). Patients who have typical symptoms should be given antitoxin and antibiotics with adequate doses. Supportive management of breathing and airway should be given if needed. 9,10
Antitoxin administration should be based on the location and size of the membrane, the degree of toxicity, and the duration of the disease (Table 1). Immediate management is essential to limit tissue damage. Adequate doses of antitoxin should be given intravenously as quickly as possible to neutralize free toxin. Sensitivity testing (diphtheria antitoxin) should be performed before administration; intradermally 0.02-0.1 mL of antitoxin serum diluted with 0.9% NaCl 1:100. Positive results if swelling occurs within 10-30 minutes. If there is no reaction, antitoxin serum can be given simultaneously intravenously. Administration of ADS intravenous in solution salt physiological or 100 mL glucose 5% in 1-2 hours. Possible effects side drug/reaction observed during giving antitoxin and the next 2 hours. It is also necessary to consider the occurrence of a delayed hypersensitivity reaction (serum disease). If there is a history of allergy, it must be decided whether the serum will still be given. If it must still be given, desensitization can be used; provide ready-to-use epinephrine 1:1000 in a syringe to anticipate anaphylactic reactions. 9.35
Table 2. Dose ADS by location membrane And long illness. 9,10
Diphtheria Types | Dose ADS (IU) | Method Giving |
Diphtheria Nose | 20,000 | Intramuscular |
Diphtheria Tonsil | 40,000 | Intramuscular or intravenously |
Diphtheria Pharynx | 40,000 | Intramuscular or intravenously |
Diphtheria Larynx | 40,000 | Intramuscular or intravenously |
Combination location in on | 80,000 | Intravenous |
Diphtheria + complications and/or found bullneck | 80,000 – 100,000 | Intravenous |
Late get medical treatment (>72 hours), the location where | 80,000 – 100,000 | Intravenous |
Patients must have total bed rest and food must be adjusted to the patient's condition. Evaluation, especially respiratory status, must be done at least every 3 hours by a nurse and 2 times a day. by doctor. Patient must placed near nurse, so that obstruction airway obstruction can be detected as soon as possible. Intubation or tracheostomy is performed if there are signs of airway obstruction accompanied by restlessness. Another alternative is orotracheal intubation, but it can cause the membrane to come off, thus failing to reduce the obstruction. Serial electrocardiogram (ECG) examinations should be 2 or 3 time a week during 4-6 Sunday For detection myocarditis as early as maybe. In disease heavy, can be given prednisone 1-1.5 mg/kg/day during 2 weeks to prevent myocarditis. Hydration status should be maintained and provide a soft or liquid diet high in calories. Secretions should be cleared by suction to prevent aspiration. Examination of voice quality and cough reflex should be done periodically to determine the progression of the disease. Other diseases may require tracheostomy to relieve obstruction. 9,10
Complications
During phase I diphtheria, myocarditis has associated with 60–70% death. DT causes myocardial dysfunction as well as bradyarrhythmias, tachyarrhythmias, and complete heart block. Conduction system disorders are a sign of myocardial damage that critical consequence inflammation I on node sinoatrial And atrioventricular which can be fatal, despite cardiac pacing. Post-diphtheria complications such as cardiomyopathy and neuropathy may occur due to autoimmune inhibition of epidermal growth factor receptor (EGFR) function, due to the similarity of antigenic epitopes between the B subunit of DT and the extracellular domain of EGFR, and this inhibition may damage host tissues expressing EGFR123. Post-diphtheria neuropathy manifests with palatal paralysis, limb weakness, and the need for mechanical ventilation in most pediatric cases. Hypoxic neurologic injury has been observed in some cases. In a study model animal, the disappearance fiber nerve in a way total observed as effect long term . 24
Studies by Kumar et al. Show 24 (72.7%) from 33 patient experiencing complications, in among others complications heart And disturbance breathing is complications Which most general And seen on 15 case (45.5%) respectively, followed by by paralysis palatal on 24.3% case, polyneuropathy on 21% cases, and bleeding or disseminated intravascular coagulation (DIC) in 21% of cases. Nine percent patient experience fail kidney I, 3% patient experience seizures, and 3% experienced septicemia. Of the 15 cases that experienced respiratory distress, 12 (80%) patient must given support ventilation. From 12 case, 7
(58.3%) patient die temporary 5 (41.7%) case endure life. Six (40%) patients undergo tracheostomy And One patient can in decannulation. From six the patient who undergo tracheostomy, two (33.3%) patient endure life And four (66.6%) died. As many as 15 (83.3%) from 18 patient Which No immunized experienced complications, 11 (61%) of whom died. Of the 10 partially immunized patients, 8 (80%) cases experienced complications and 3 (30%) of whom died. Meanwhile, of the five immunized patients, only one (20%) experienced complications, And four the rest own journey disease Which were not too severe and all five (100%) patients survived. 26 The study is in line with studies by Meshram et al. and Ujwal et al. who showed myocarditis as the most common complication, namely 42.5 and 63.3% respectively. 36,37
The most common complication in cases of diphtheria is neurological, where paralysis palatal is manifestation clinical Which most general, followed by motor weakness and uncommon cases of paralytic ileus and bilateral abductor paralysis with facial nerve palsy. Palatal paralysis is characterized by a nasal voice quality, nasal regurgitation is common on Sunday second And third And is complications neurological earliest complication that can occur alone or in association with other types of paralysis. The exact mention of paralytic ileus is not found in the literature but may be related to the fact that the parasympathetic fibers to the intestines and bladder are located more medially in the spinal cord and are, therefore, the last to be affected by the pathological process. The second most common complication of diphtheria is myocarditis. Myocarditis occurs due to exotoxins bacteria that cause DNA fragmentation and cytolysis by inhibiting the activity of elongation factor-2 in protein synthesis in addition to damage to the conducting tissue. It has been shown to be associated with the highest mortality rate. 38
Prevention
Community-based diphtheria prevention is most effective through active immunization. Primary diphtheria immunization is given together with tetanus toxoid and pertussis vaccine. in form DPT vaccine three times with interval 4-6 weeks. Basic DPT immunization (DPT-1, DPT-2, and DPT-3) is given 3 times from the age of 2 months (not may before the age of 6 week) with interval 4-8 weeks. DPT booster repeat immunization (DPT-4) is given one year after DPT-3 (age 18-24 months) and DPT-5 when entering school at the age of 5 years. If at the age of 5 years DPT-5 has not been given, the booster vaccination is given Td according to the School Children's Immunization Month program (BIAS, Elementary School grade 1, age 7 years). Td booster vaccination given 2 times on program BIAS (SD class 2 And 3). Dose DPT vaccination (DTWP, DTaP, DT, or Td) is 0.5 mL intramuscularly for both primary and booster immunizations. 9,10
CONCLUSION
Tonsillitis is a common disease that is usually caused by a viral infection. or bacteria, with risk infection diphtheria can increase on individual who are not immunized. 3
Diphtheria is an infectious disease that can be prevented through immunization. This disease is caused by the bacteria Corynebacterium diphtheriae and attacks the mucous membranes. mucus in area like pharynx, larynx, And tonsils., Man is the only host bacteria This, And transmission happen through droplet from channel respiratory tract or direct contact with skin lesions. The main symptoms include sore throat, difficulty swallowing, mild fever (less than 38.5°C), and a white or gray pseudomembrane in the throat. About 94% of diphtheria cases occur in the tonsils and pharynx, with severe cases showing difficulty breathing. Death can occur from airway obstruction or damage to the heart and nervous system. Infection in location pharynx produces symptoms beginning in the form of malaise, sore throat, anorexia, and increased pseudo membrane, dangerous if a burst of toxins occurs in the patient's body. 5
Diphtheria tonsillitis can be diagnosed based on anamnesis, physical examination And inspection support. Inspection support like culture swab throat, nose And checked in laboratory, inspection toxin diphtheria can also be done by using the ELEK test.
Prevention of diphtheria can be done through diphtheria vaccination. This given in form combination with vaccine tetanus And pertussis (DPT), wash hand with soap And water flow, avoid contact with diphtheria tonsillitis sufferers, using masks when around sufferers and increasing public awareness about diphtheria tonsillitis. 16
REFERENCE
Bukhari HQ, Madloul MH, Alorinan BI, et al. Prevalence Study Of Acute Tonsillitis Among Pediatric Age Groups. International Journal of Medical Reviews and Case Reports. 2019:1-5.
Anderson J, Paterek E. Tonsillitis. [Updated 2023 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK544342/
Alghamdi RM, Alzahrani RA, Alzahrani AAH, et al. Tonsillitis Prevalence, Diagnosis, and Treatment among Patients at Al-Baha Region, Saudi Arabia. Saudi Journal for Health Sciences. 2023;12(3):227-234.
Chaudhary A, Pandey S. Corynebacterium diptheriae . [Updated 2023 Jun 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-
True Love SA, Keegan LT, Moss WJ, et a. Clinical and Epidemiological Aspects of Diphtheria: A Systematic Review and Pooled Analysis. Clin Infect Dis. 2020;71(1):89-97.
Noor AB, et al. Clinical spectrum and outcomes of the 2019-2020 pediatric diphtheria outbreak in Yemen. Indonesian Paediatr. 2024;64(1):36-43.
Ikejezie J, Adebusoye B, Ekezie W, Langley T, Lewis S, Phalkey R. Modifiable risk factors for diphtheria: A systematic review and meta-analysis. Glob Epidemiol. 2023;5:100100.
Sampealang MP, Anggara A, Faris A. Diphtheria in Children. Journal of Medical Profession (MedPro). 2021;3(2):130-135.
Saunders R, Suarca IK. Diagnosis and Management of Diphtheria. CDK. 2019;46(2):98-101.
Ministry Health Republic Indonesia. Guidelines Prevention And Diphtheria Control . Ministry of Health of the Republic of Indonesia. 2017. Available from: https://sehatnegeriku.kemkes.go.id/wp-content/uploads/2018/01/buku- diphtheria-prevention-and-control-guidelines.pdf
Singh A, Prasad R, Sharma IK, Agarwal P, Gemini, Sharma N. Diphtheria in Western Uttar Pradesh: A Re-emerging Threat. Pediatr Infect Dis J. 2022;41(11):e499-e500.
Murhekar M. Epidemiology of Diphtheria in India, 1996-2016: Implications for Prevention and Control. Am J Trop Med Hyg. 2017;97(2):313-318.
Clarke KEN, MacNeil A, Hadler S, Scott C, Tiwari TSP, Cherian T. Global Epidemiology of Diphtheria, 2000-20171. Emerg Infect Dis. 2019;25(10):1834- 1842.
Ministry of Health of the Republic of Indonesia. Indonesian Health Profile 2021. Ministry of Health of the Republic of Indonesia. Jakarta. 2021.
Ministry of Health of the Republic of Indonesia. Indonesian Health Profile 2023. Ministry of Health of the Republic of Indonesia. Jakarta. 2023.
. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559015/Sari N, et al. Epidemiological Investigation of Diphtheria Cases in Kediri Regency in 2022. Wiyata Journal, 2023;10(01):82-90.
Lamichhane A, Radhakrishnan S. Diphtheria. [Updated 2024 Feb 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560911/
Workmanship MR, Nelwan EJ, Assyidiqie IZ, Satari HI, Hadinegoro SR. Diphtheria Epidemiology in Indonesia during 2010-2017. Acta Med Indonesia. 2019;51(3):205-213.
Rintani A, et al. Risk Factor Associated to Diphtheria Outbreak In Developing Countries. Journal of Public Health Sciences, 2018;9(2):83-95.
Nassar Oh my, Abdullah Al-Amad M, Ghaleb YES. Risk factors for diphtheria in Sana'a, Yemen, 2019: a matched case-control study. IJID Reg. 2021;2:40-44.
Dureab F, Al-Sakkaf M, Ismail O, et al. Diphtheria outbreak in Yemen: the impact of conflict on a fragile health system. Confl Health. 2019;13:19.
Hoskins PA. Microbes Profile: Corynebacterium diphtheria - an old foe always ready to seize opportunity. Microbiology (Reading). 2018;164(6):865-867.
Ott L, Möller J, Burkovski A. Interactions between the Re-Emerging Pathogen Corynebacterium diphtheria and Host Cells. International Journal of Molecular Sciences. 2022; 23(6):3298.
Sharma NC, Efstratiou A, Mokrousov I, Mutreja A, Das B, Ramamurthy T. Diphtheria. Nat Rev Dis Primers. 2019;5(1):81.
Arguni E, Karyanti MR, Satari HI, Hadinegoro SR. Diphtheria outbreak in Jakarta and Tangerang, Indonesia: Epidemiological and clinical predictor factors for death. PLOS One. 2021;16(2):e0246301.
Kumar L, et al. Clinical Profile and Predictors of Outcome in Patients with Diphtheria in a Tertiary Care Center. Otorhinolaryngology Clinics: An International Journal. 2021;13(3):77-81.
Singh S, Gupta N, Saple P. Diphtheritic myocarditis: A case series and review of literature. J Family Med Prim Care. 2020;9(11):5769-5771.
UK Health Security Agency. Public health control and management of diphtheria in England: 2023 guidelines. 2023. Available from: https://assets.publishing.service.gov.uk/media/654944a9bdb7ef000d4af91c/dip htheria-guidelines-version19-November2023.pdf
Aboul-Enein BH, Puddy WC, Bowser JE. The 1925 Diphtheria Antitoxin Run to Name - Alaska: A Public Health Illustration of Human-Animal Collaboration. J Med Humanit. 2019;40(3):287-296.
Prygiel M, Mosiej E, Polak M, Krysztopa-Grzybowska K, Wdowiak K, Formińska K, Zasada AA. Challenges of Diphtheria Toxin Detection. Toxins. 2024; 16(6):245.
Melnikov VG, Berger A, Sing A. Detection of diphtheria toxin production by toxigenic corynebacteria using an optimized Elek test. Infection. 2022;50:1591– 1595.
Simonova MA, Melnikov VG, Lakhtina OE, et a. Determination of Diphtheria Toxin in Bacterial Cultures by Enzyme Immunoassay. Diagnostics (Basel). 2022;12(9):2204.
Dincer C, Bruch R, Costa-Rama E, et al. Disposable Sensors in Diagnostics, Food, and Environmental Monitoring. Adv Mater. 2019;31(30):e1806739.
Sivakumar R, Lee NY. Recent advances in airborne pathogen detection using optical and electrochemical biosensors. Anal Chim Acta. 2022;1234:340297.
Hartoyo E. Diphtheria on child. Sari Pediatrics. 2018;19(5):300–6.
Meshram RM, Patil A. Clinical profile and outcome of diphtheria in central India: a retrospective observational study. Int J Contemp Pediatr. 2018;5(4):1600-1605.
Ujwal MV, Pol RR, Vanaki R, et al. Resurgence of diphtheria in rural north Karnataka: clinical profile and outcome. Int J Med Paediatr Oncol 2019;5(1):17–20.
Sharma S, Jammar S, Kataria T, et al. An Observational Study on Association of Clinical Outcome of Diphtheria Cases with Immunization Status: A Tertiary Care Hospital, Jaipur. Indian J Otolaryngol Head Neck Surg. 2022;74(Suppl 3):5460-5464.
sfasfasfa
Comments